
Christmas lockdown: Javid does not rule out new restrictions


They do seem to offer significant protection against severe illness, but the consequences of rapidly spreading infection worry many public health experts.A growing body of preliminary research suggests the Covid vaccines used in most of the world offer almost no defense against becoming infected by the highly contagious Omicron variant.All vaccines still seem to provide a significant degree of protection against serious illness from Omicron, which is the most crucial goal. But only the Pfizer and Moderna shots, when reinforced by a booster, appear to have success at stopping infections, and these vaccines are unavailable in most of the world.The other shots — including those from AstraZeneca, Johnson & Johnson and vaccines manufactured in China and Russia — do little to nothing to stop the spread of Omicron, early research shows. And because most countries have built their inoculation programs around these vaccines, the gap could have a profound impact on the course of the pandemic.A global surge of infections in a world where billions of people remain unvaccinated not only threatens the health of vulnerable individuals but also increases the opportunity for the emergence of yet more variants. The disparity in the ability of countries to weather the pandemic will almost certainly deepen. And the news about limited vaccine efficacy against Omicron infection could depress demand for vaccination throughout the developing world, where many people are already hesitant or preoccupied with other health problems.Most evidence so far is based on laboratory experiments, which do not capture the full range of the body’s immune response, and not from tracking the effect on real-world populations. The results are striking, however.The Pfizer and Moderna shots use the new mRNA technology, which has consistently offered the best protection against infection with every variant. All of the other vaccines are based on older methods of triggering an immune response.The Chinese vaccines Sinopharm and Sinovac — which make up almost half of all shots delivered globally — offer almost zero protection from Omicron infection. The great majority of people in China have received these shots, which are also widely used in low-and middle-income countries such as Mexico and Brazil.A preliminary effectiveness study in Britain found that the Oxford-AstraZeneca vaccine showed no ability to stop Omicron infection six months after vaccination. Ninety percent of vaccinated people in India received this shot, under the brand name Covishield; it has also been widely used across much of sub-Saharan Africa, where Covax, the global Covid vaccine program, has distributed 67 million doses of it to 44 countries.Workers unloaded a shipment of China’s Sinopharm vaccine in Bujumbura, Burundi. China’s Sinopharm and Sinovac vaccines together make up almost half of all the shots delivered globally.Tchandrou Nitanga/Agence France-Presse — Getty ImagesAdministering the AstraZeneca shot in Milan.Alessandro Grassani for The New York TimesResearchers predict that Russia’s Sputnik vaccine, which is also being used in Africa and Latin America, will show similarly dismal rates of protection against Omicron.Demand for the Johnson & Johnson vaccine had been surging in Africa, because its single-shot delivery regimen makes it easy to deliver in low-resource settings. But it too has shown a negligible ability to block Omicron infection.Antibodies are the first line of defense induced by vaccines. But the shots also stimulate the growth of T cells, and preliminary studies suggest that these T cells still recognize the Omicron variant, which is important in preventing severe disease.“What you lose first is protection against asymptomatic mild infection, what you retain much better is protection against severe disease and death,” said John Moore, a virologist at Weill Cornell Medicine in New York. He called it “a silver lining” that Omicron so far appears less lethal than the Delta variant.But this protection will not be enough to prevent Omicron from causing global disruption, said J. Stephen Morrison, director of the Global Health Policy Center at the Center for International and Strategic Studies.“The sheer scale of infection will overwhelm health systems, simply because the denominator will be potentially so big,” he said. “If you have a burst of infection worldwide, a shock, what does the world look like on other side of it? Is it, ‘The war is over,’ or, ‘The war has just entered another phase’? We haven’t begun thinking about any of that.”People with breakthrough cases may experience only asymptomatic infection or mild illness, but they can pass the virus to unvaccinated people, who could fall more severely ill, and become a source of new variants.A Sinovac vaccination in Cachoeira do Piria, Brazil, in January. Experts fear news of limited vaccine efficacy against Omicron will depress demand for vaccination in places where people are already hesitant.Tarso Sarraf/Agence France-Presse — Getty ImagesMonks signed up for AstraZeneca’s shot in Bangkok in April.Adam Dean for The New York TimesDr. Seth Berkley, the chief executive of Gavi, the global vaccine alliance, said that more data was needed before drawing conclusions about vaccines’ effectiveness against Omicron — and that accelerated vaccination should continue to be the focus of pandemic response.Preliminary data from South Africa suggest that with Omicron, there is a much higher chance of people who already had Covid getting reinfected than there was with the original virus and previous variants. But some public health experts say they believe that countries that have already been through brutal waves of Covid, such as Brazil and India, may have a buffer against Omicron, and vaccination after infection produces high antibody levels.“The combination of vaccination and exposure to the virus seems to be stronger than only having the vaccine,” said Ramanan Laxminarayan, an epidemiologist in New Delhi. India, he noted, has an adult vaccination rate of only about 40 percent but 90 percent exposure to the virus in some areas.“Without a doubt Omicron is going to flood through India,” he said. “But hopefully India is protected to some extent because of vaccination and exposure.”China does not have this layer of protection to back up its weak vaccines. Because of China’s aggressive efforts to stop spread of the virus within its borders, relatively few people have previous exposure. Only an estimated 7 percent of people in Wuhan, where the pandemic began, were infected.Much of Latin America has relied on the Chinese and Russian vaccines, and on AstraZeneca. Mario Rosemblatt, a professor of immunology at the University of Chile, said that more than 90 percent of Chileans had had two doses of one vaccine, but the great majority of these were Coronavac, the Sinovac shot. High vaccination coverage combined with early reports that Omicron does not cause serious illness is leading to a false sense of security in the country, he said.The Coronavirus Pandemic: Key Things to KnowCard 1 of 4A new U.S. surge.
Read more →
SharecloseShare pageCopy linkAbout sharingImage source, Getty ImagesThe Netherlands has announced a strict lockdown over Christmas amid concerns over the Omicron coronavirus variant. Non-essential shops, bars, gyms hairdressers and other public venues will be closed until at least mid-January. Two guests per household will be allowed – four over the holidays.Prime Minister Mark Rutte said the restrictions were “unavoidable”. Countries across Europe have been tightening restrictions as the heavily mutated variant spreads. The new rules in the Netherlands – the strictest to have been announced over Omicron so far – come into force on Sunday.”I stand here tonight in a sombre mood. And a lot of people watching will feel that way too,” Mr Rutte told a news conference on Saturday. “To sum it up in one sentence, the Netherlands will go back into lockdown from tomorrow.”Under the new rules, people are being urged to stay at home as much as possible. Strict limits will be placed on the number of people who can meet – a maximum of two guests over the age of 13 will be allowed in people’s homes, and four on 24-26 December and on New Year’s Eve. All schools will be closed until at least 9 January, while other lockdown measures will remain in place until at least 14 January. The BBC’s Anna Holligan in The Hague said the announcement was being met with disbelief and dismay. For weeks, curfews have been placed on hospitality and cultural venues in the Netherlands an effort to limit the spread of Omicron. The Dutch National Institute for Public Health has reported more than 2.9m coronavirus cases since the pandemic began, and over 20,000 deaths. It says the Omicron variant currently still accounts for a minority of coronavirus cases in the Netherlands but is spreading rapidly. Officials say it is expected to become the dominant variant by the New Year.Mr Rutte said a failure to act now would likely lead to “an unmanageable situation in hospitals”. At the news conference on Saturday, officials urged people to get vaccinated.
Read more →
After she and her husband attended a Masters and Johnson lecture in 1966, they joined the burgeoning field of sexology. She remained active well into the 21st century.Shirley Zussman, a sex therapist who was trained by William H. Masters and Virginia E. Johnson, the researchers who demystified the mechanics of sex, and who continued seeing patients until she was 105, died on Dec. 4 at her home in Manhattan. She was 107.Her son, Mark Zussman, confirmed the death.In 1966, Dr. Zussman, a psychiatric social worker and psychotherapist, and her husband, Leon Zussman, a gynecologist and obstetrician, were invited to a lecture given by two sex researchers who were virtually unknown at the time: Dr. Masters, a gynecologist, and Ms. Johnson, a college dropout who had studied psychology.At their St. Louis clinic, the couple (Dr. Masters was at the time married to someone else) had begun helping people improve their sex lives, using what they’d learned in nearly a decade of clinical research studying the ways men and women had sex and what gave them pleasure. Their book “Human Sexual Response,” which popularized the treatment of sexual dysfunction and helped liberate its sufferers from the analyst’s couch, had just been published and was not yet the runaway best seller it would become. But the lecture they delivered, as Dr. Zussman told Time magazine in 2014, the year of her centennial, resonated for her and her husband.Dr. Masters and Ms. Johnson’s research found that women could be multi-orgasmic, but not always or often — or, in some cases, ever — through penetration. They were pro-masturbation and taught about it. It was a fraught cultural moment, as the buttoned-up 1950s gave way to what Dr. Zussman called the frantic hookups of the ’60s, and each period had in its own way had been a recipe for performance anxiety and distress.Despite the relaxing mores of the ’60s, Dr. Zussman recalled: “It was all not just glamorous and wonderful to be sexual. One had to almost learn how to be a good partner and to enjoy the pleasure, not only for yourself but for each other. And I thought, ‘We can do that! Why can’t we do that?’”The Zussmans trained at the Masters and Johnson Institute and by the mid-’70s were co-directors of the Human Sexuality Center at Long Island Jewish-Hillside Medical Center. Their patients were married couples, typically women who were not orgasmic and men who were impotent or ejaculating prematurely.They felt the underlying issues had to do with communication, as they gently detailed in their 1979 book, “Getting Together: A Guide to Sexual Enrichment for Couples.” With exercises both physical and psychological — the Zussmans encouraged their patients to plumb their upbringing for clues to their attitudes about sex and relationships, and to examine how work, family and societal pressures affected their intimacy — the book was wide-ranging in its scope. It was also compassionate.The book that Dr. Zussman and her husband, Leon, published in 1979 aimed to teach couples how to communicate better. “Shirley was a pioneer in sex therapy and an excellent role model,” said Ruth Westheimer, who was a program director at Planned Parenthood and was studying sexuality at Columbia University when she took a course in sex therapy taught by Dr. Zussman and her husband at their Long Island clinic. It was the first experience with the discipline for Dr. Westheimer, the buoyant Holocaust survivor and sexologist who later became a familiar face on television. “They were trailblazers, because she was a therapist and her husband was a gynecologist and that validated the work. It gave it the legitimacy that sex therapists like me needed. I wouldn’t be talking about orgasms if it wasn’t for Shirley.”Sexual pleasure, Dr. Zussman said in 2014, “is only one part of what men and women want for each other. They want intimacy. They want closeness. They want understanding. They want comfort. They want fun. And they want somebody who really cares about them beyond going to bed with them. And I think people are always seeking that in every generation.”Shirley Edith Dlugasch was born on July 23, 1914, on the Lower East Side of Manhattan. Her father, Louis Dlugasch, was a doctor, and her mother, Sara (Steiner) Dlugasch, was a surgical nurse.Shirley grew up in Brooklyn and attended Smith College, majoring in psychology and graduating in 1934. (Julia Child was classmate.) She earned a diploma at the New York School of Social Work-Columbia University (now the Columbia School of Social Work) in 1937, and a doctorate in education from Teachers College, at Columbia University in 1969.Her dissertation looked at husbands who were present in the delivery room, a radical act in the ’50s and ’60s. Dr. Zussman wanted to explore delivery customs in other cultures, and she reached out to the celebrated anthropologist Margaret Mead, who was a member of Columbia’s faculty, to be on her thesis committee.In addition to her son, Dr. Zussman is survived by her daughter, Carol Sun; three grandchildren; two step-grandchildren; and seven great-grandchildren. Leon Zussman died in 1980.Shirley and Leon Zussman in an undated photo.They had a sex therapy practice together and were directors of a clinic in Long Island. via Zussman familyDr. Zussman was twice president of the American Association of Sex Educators, Counselors and Therapists. She was a frequent guest on talk shows and for a decade and a half had a monthly column in Glamour magazine, “Sex and Health,” She attributed her long life to good genes: Her sister lived to 104, her brother to 96.In her practice of both sex therapy and psychotherapy, Dr. Zussman saw same-sex couples and single people as well as heterosexual couples. She said the most common problem among her patients in the 21st century was a lack of desire.“You have to look at your priorities,” she told Time magazine. “You have to decide what is important to make you feel good about yourself and your life. And to help make your partner feel good. To establish something that is gratifying, that fills a need that we all have to be close to somebody.”
Read more →
A major incident has been declared in London and more than 10,000 Omicron new cases have been found in the UK, as the variant surges across the country.Sadiq Khan says it’s important that Londoners understand how serious the surge in cases is.More on this story: More than 10,000 new Omicron cases found in UK
Read more →
I.V.F. patients are faced with a growing list of costly “add-ons.” For one such test, some say more robust research is needed to support its effectiveness.For patients undergoing in vitro fertilization, there is a common test to help determine the best time to transfer the embryo for a successful pregnancy. But new research has patients and doctors questioning whether the test — one of a growing number of expensive “add-ons” for I.V.F. patients — is effective for first-time patients.The test, called an endometrial receptivity analysis, takes a biopsy of the interior lining of the uterus. Then a lab analyzes the tissue for more than 200 genes to predict the best time to place the embryo in the uterus, according to the test’s manufacturer, Igenomix.The study, whose findings were published in September, compared live birthrates for first-time I.V.F. patients who had the E.R.A. to those who did not, and researchers found no difference between the two groups. In other words, the test does not improve chances of achieving an ongoing pregnancy in first-time patients, according to the findings.The research, which was sponsored by Igenomix and has not been peer-reviewed or published in full, also noted that more studies were needed to assess whether the test could be beneficial for patients who have had multiple failed transfers. The study was led by researchers from Shady Grove Fertility, which has more than 40 clinics across the United States.“It doesn’t improve the live birthrates for all women,” said Dr. Nicole Doyle, the study’s lead researcher and a reproductive endocrinologist at Shady Grove. “We had hoped for better results, but from a cost benefit, it’s not worth it,” she said of the test, which can cost patients up to $1,000.“This type of study should have been done earlier,” said Dr. Eric Forman, the medical and laboratory director at Columbia University’s Fertility Center. He said the test had been used tens of thousands of times in the United States since it became available in 2011.Some clinics offer the test for all patients, while others recommend it for those with failed cycles. Many patients request the test after reading about it in online forums. Dr. Aimee Eyvazzadeh, a reproductive endocrinologist in San Ramon, Calif., said she offered the test to all patients, and about half of her first-time patients opted to do it. “They feel so empowered by having the option,” she said.The Shady Grove study offered 767 first-time I.V.F. patients a free E.R.A. before transfer. (Genetic tests ruled out any failures involving an abnormal embryo.)The patients each had one embryo transferred; half used the test and the other half did not. The results found that just over 54 percent of the group that used the test had an ongoing pregnancy, compared with just over 63 percent of the control group.Igenomix said in an emailed statement that despite funding the research, the company had not had access to the raw data and was waiting for it to be published in a peer-reviewed journal before commenting on the results.The company, which was acquired by Vitrolife in July, said that 25 other studies — 16 internal and nine independent — supported use of the test. In reality, the existing body of data shows mixed results about the test’s effectiveness.A 2018 independent study of patients with two or fewer previous failed transfers found that the test did not improve pregnancy outcomes, but the study used only a small sample of participants.One Igenomix study from 2013 found that one in four women with repeated I.V.F. failure had a displaced window of implantation and concluded that those patients could benefit from using the test. A randomized clinical trial sponsored by the company from 2020 used a sample of mostly first-time patients, with some who had experienced up to a few failed attempts. The trial concluded that those who used the test had a “significant improvement” in live birthrates, but did not differentiate between first-time patients and those with previous failed transfers. Some scientists have also criticized the study’s methodology as flawed.The Igenomix statement said that given the latest Shady Grove study, more research was needed to determine whether the test “could be clinically useful in all patients at the first appointment.”Dr. Doyle and her team’s findings underscore critics’ ongoing concerns about the need for greater regulation of the I.V.F. industry. “It’s both irresponsible and unethical for clinics to sell I.V.F. add-ons that are scientifically unproven,” said Pamela Mahoney Tsigdinos, a patient advocate and the author of “Silent Sorority.”While the test is certified and regulated by the Centers for Medicare and Medicaid Services, it is not approved by the Food and Drug Administration. The E.R.A. is considered a laboratory-developed test, according to Igenomix, a category that can bypass F.D.A. scrutiny. (This same loophole allowed Theranos, the blood testing start-up founded by Elizabeth Holmes, to evade the agency’s oversight. Ms. Holmes is on trial for fraud charges.)I.V.F. is a costly endeavor with no guarantee of success. A single I.V.F. cycle can exceed $20,000, according to data from FertilityIQ, a company that provides reviews of fertility clinics. Most people need at least three to four I.V.F. cycles to be successful.There were almost 330,000 assisted reproductive technology cycles (which includes I.V.F. and egg freezing) performed in the United States in 2019, according to preliminary data from the Centers for Disease Control and Prevention, with nearly 78,000 patients giving birth.“I.V.F. has reached maturity as a technology and we’re approaching the limits of its efficacy,” said Dr. Andrea Vidali, a reproductive immunologist and repeat miscarriage specialist in New York.He believes add-ons like the E.R.A. are a result of an industry focused on “troubleshooting I.V.F. failure.” He said that doctors adopted the test because “patients don’t want to be told they have unexplained infertility when they ask for a reason as to why their I.V.F. transfer failed, and they are looking for answers.”Patients undergoing I.V.F. are presented with a list of add-ons “with no ability” to assess the value, according to David Sable, a venture capital fund manager and reproductive endocrinologist.In light of the new research, some fertility doctors are reconsidering the test’s use on first-time patients, while other doctors are further dissuaded from using it at all.“We have always discouraged the E.R.A. test,” said Dr. Peter Klatsky, a founder of Spring Fertility, which has clinics in California, New York and Vancouver. He has observed the test’s popularity grow in recent years. “This study makes it easier to explain why we do not recommend this test when patients have read positive testimonials online,” he said.Some patients who had ongoing pregnancies after using the test are now unsure of whether their success was a result of the test.Nathalie Carpenter, the 42-year-old founder of a wellness marketing agency and a community advocate for infertility in Connecticut, received the test ahead of two I.V.F. cycles, each years apart. The first resulted in a daughter; the second failed. She wonders now whether the E.R.A. was effective. But at the time, she said, “I trusted my doctor; I didn’t question it.”Some patients remain hopeful that the test could tip the scale toward a successful pregnancy regardless of the ambiguous data.When Rhian Thomas, a 39-year-old television producer in New York, was preparing for her first embryo transfer at the Columbia University Fertility Center, she told Dr. Forman, the center’s medical and laboratory director, that she wanted an E.R.A., even though he was skeptical.Having experienced multiple miscarriages before, Ms. Thomas said she wanted to “go through every test on the planet” for the best chance of pregnancy. The transfer after the test resulted in a son, who is now seven months old.Despite the new study, Ms. Thomas said she was glad she did the test and would do it again. “If it didn’t work out, I would wonder, ‘What if the implantation window was off?’” she said. “You want control. And that’s what the E.R.A. does — it gives an element of control over these things.”
Read more →
Omicron has cast a shadow over holiday plans.Is Omicron really going to ruin Christmas?Ever since Covid-19 cases began rising sharply, long-awaited plans to see friends and relatives have suddenly been called into question. We want to see one another — but should we?So far it appears as though Omicron won’t make a dent in holiday travel. AAA estimates that more than 109 million Americans will travel during the Christmas and New Year’s holiday season, a 34 percent increase from 2020.But Omicron appears to be the most contagious variant yet. Should we worry about visiting older relatives? Is flying considered safe? What about Christmas dinner?We asked three epidemiologists and a psychologist to help untangle these and other complicated questions, and offer tips on staying safe. Here is their guidance.Is plane travel OK?On Friday, Dr. Anthony Fauci, the nation’s top infectious disease expert, said on CNBC that despite Omicron, those who are vaccinated “and hopefully also boosted” should feel “reasonably comfortable” enjoying the holidays at a family member’s home, and that he “would not hesitate” to get on a plane if he had to.But “the risk is never zero, that’s for sure,” he added.In the end, the answer depends on your personal tolerance for risk and how important the trip is to you.Experts say it is crucial to rely on a layered approach to lowering risk, namely: getting vaccinated, getting a booster shot if eligible, wearing a mask, having proper ventilation and using rapid home testing.Katelyn K. Jetelina, an assistant professor of epidemiology at the University of Texas Health Science Center at Houston, is traveling to California on Sunday with her two young girls, 2 and 14 months. She is prepared to cancel their flight at a moment’s notice if she and her husband start to feel uneasy. So far, however, she isn’t overly concerned about air travel.“I would consider it a low risk because of filtration systems and ventilation, as well as masks are required — not only that, they’re enforced,” she said.If people on the plane are taking off their masks for extended periods of time for snacks or meals, that increases the risk of infection for everyone on that plane, she added. So she advised leaving your mask on. “Masks protect the wearer, too,” she said. “Not just the people around them.”Dr. Jetelina recommends upgrading to an N95 mask, if you haven’t already. For children, she suggests KN95s because N95s don’t come in their sizes.Many public health experts recommend the KF94 mask, which is made in South Korea, because of its quality, high filtration rate and snug fit.When asked about masks on Friday, Dr. Fauci said that while the N95 was the best mask at blocking aerosol and droplet particles, they can be relatively uncomfortable to wear. “A regular surgical mask as well as a cloth mask is fine,” he added.Getting to and from the flight creates additional risk because the trip adds more opportunities for exposure. So instead of taking a car service, Dr. Jetelina has asked her vaccinated relatives to come to the airport and pick her and her family up.Her family is also aiming to minimize exposure to indoor crowds, especially in places that may have poor ventilation. Either she or her husband will take the children outside while the others wait at baggage claim, for example.Dr. Michael Mina, a former Harvard epidemiologist who is now the chief science officer for eMed, a company that verifies at-home test results, said he plans to fly to Colorado this month with his wife and 2-month-old daughter.“This isn’t going to be the last variant, and I think that we have the ability to gather safely if we do it right,” he said.How can rapid tests help us?Rapid antigen tests, which can indicate within minutes whether someone is contagious with Covid-19, are one of the best ways to help ensure everyone’s safety this holiday season, the experts said.The tests remain expensive — a typical two-pack costs $14 to $24 — and sometimes they can be hard to track down in stores. But if you’re fortunate enough to have some on hand, Dr. Mina suggests that everyone test 15 minutes before gathering. It’s important to do the test in a room-temperature setting like a car, he added, because the tests lose some of their efficacy if they are conducted in temperatures below 55 degrees.Dr. Jetelina and her family will be using the tests right before heading to the airport, once they land and then every other day before their family members gather for Christmas.If your test is negative, you can feel reassured that you are not infectious at that moment. Because the tests function as a snapshot in time, taking one on the day before a gathering isn’t useful.The Coronavirus Pandemic: Key Things to KnowCard 1 of 4A new U.S. surge.
Read more →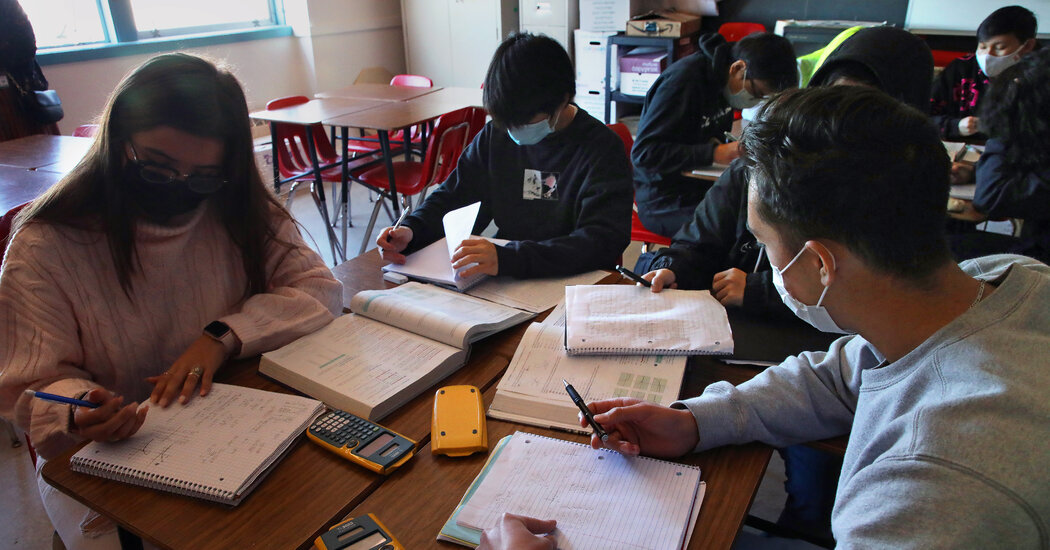
Two new studies show that unvaccinated children exposed to the virus are safe to stay in school if they remain asymptomatic and get tested twice over the course of a week.WASHINGTON — The Centers for Disease Control and Prevention said on Friday that unvaccinated students exposed to the coronavirus can remain in school, as long as they are tested for the virus twice in the week after and both tests come back negative.The new guidance, known as the “test-to-stay” protocol, could ease the burden on children who have been expected to stay home if a close contact tested positive for the virus, and on parents who have had to scramble to retrieve them from school or find day care. It also aims to minimize disruptions to learning as two highly contagious variants of the virus spread across the country, causing some school closures and threatening to upend the strategies that federal and state officials adopted to return to in-person classes in the fall.Although some schools and districts are already using the test-to-stay approach, the C.D.C. had not previously endorsed it, citing a lack of evidence. On Friday, the agency released studies from two counties, one in California and the other in Illinois, that effectively tested the protocol and found that it worked.The studies were conducted before the fast-moving Omicron variant began spreading in the United States. Scientists are still investigating many basic questions about the variant, including whether it increases the risk of in-school transmission.“Even with the recent increase in Omicron variant, we expect that these prevention strategies will continue to work,” Kristen Nordlund, a C.D.C. spokeswoman, said in a statement on Friday. “However, as we learn more about the Omicron variant, C.D.C. will continue to review and update guidance as needed.”The new policy, hinted at in the winter Covid-19 plan that President Biden unveiled this month, still calls on students to wear masks and socially distance, and applies only to those who remain asymptomatic. Until now, unvaccinated students were expected to quarantine at home for as long as two weeks after exposure. Some states have had tens of thousands of students in quarantine.“While over 99 percent of schools are open now, we need to make sure we keep that throughout the winter,” Mr. Biden said as he announced the plan. “We want our children in school.”Vaccinated students with exposures have generally been allowed to remain in school as long as they are asymptomatic and wear a mask. Dr. Rochelle P. Walensky, the C.D.C. director, said at a news conference on Friday that students participating in test-to-stay programs should be tested at least twice during the seven-day period after an exposure.In one of the studies the C.D.C. released on Friday, students at schools in Los Angeles County that did not participate in a pilot test-to-stay program, and who had to quarantine, lost an estimated 92,455 in-person school days from Sept. 20 to Oct. 31. In schools participating in the pilot, students exposed to the virus lost no days. Those schools also did not see increases in virus rates among students.In Lake County, Illinois, where the other study took place, researchers estimated that up to 8,152 in-person learning days were saved from August to October in schools that participated in the program. Of the 16 students in the program who tested positive for the virus in the two weeks after exposure, none appeared to transmit it to others at school, the report said.The California students were tested twice in the week after exposure; the Illinois students were tested four times.Dr. Walensky said on Friday that the protocol was “now proven.” She added that because “test to stay” had only been studied in schools, the C.D.C. did not yet have evidence about its effectiveness in other settings.Other studies have suggested the test-to-stay approach can be safe. One randomized controlled trial included more than 150 schools in Britain, and found that case rates were not significantly higher at schools that allowed close contacts of infected students or staff members to remain in class with daily testing than at those that required at-home quarantines.The Coronavirus Pandemic: Key Things to KnowCard 1 of 4A new U.S. surge.
Read more →
As our brains age, small lesions begin to pop up in the bundles of white matter that carry messages between our neurons. The lesions can damage this white matter and lead to cognitive deficits. Now, researchers at Stevens Institute of Technology and colleagues not only provide an explanation for the location of these lesions but also how they develop in the first place.
The work, led by Johannes Weickenmeier, an assistant professor of mechanical engineering at Stevens, highlights the importance of viewing the brain as more than neural circuitry that underpins how thoughts are formed, and memories created. It’s also a physical object that’s prone to glitches and mechanical failures. “The brain is susceptible to wear and tear in vulnerable areas,” Weickenmeier said. “Especially in an aging brain, we need to look at its biomechanical properties to better understand how things can start to go wrong.’
These lesions — known as deep and periventricular white matter hyperintensities because they show up as bright white patches on MRI scans — are poorly understood. But they are not uncommon: most people have some by the time they reach their 60s, and changes only increase with age. The more lesions that accumulate and the faster they grow, the more prone we become to cognitive impairments ranging from memory problems to motor disorders.
Using MRI scans from eight healthy subjects, Weickenmeier worked with Valery Visser, now a doctorate student at the University of Zurich, and Henry Rusinek, a radiologist at NYU Grossman School of Medicine, to develop an individualized computer model of each subject’s brain. The team mapped the strain placed on ventricular walls, the linings of fluid-filled chambers deep in the brain, as waves of pressure pulse through the subject’s cerebral spinal fluid, or CSF. They found that hyperintensities tend to occur near areas that must stretch more to accommodate pressure changes of the circulating CSF because, as such areas wear thin, CSF can leak into the brain and cause lesions.
“The cell wall that lines the ventricles wears out over time, like a balloon that’s repeatedly blown up and deflated,” said Weickenmeier. “And the stresses aren’t uniform — they’re defined by the geometry of the ventricle, so we can predict where these failures will occur.”
The model provides a simple, physics-based explanation for the locations of these lesions, revealing that mechanical loads “must be a major contributor to the onset of disease,” said Weickenmeier.
The team’s research, published recently in Scientific Reports, used 2D imaging showing a cross-section of the brain, but Weickenmeier’s team has since expanded its research to a full 3D model of the brain. Next, Weickenmeier hopes to use advanced MRI technologies developed at Stevens to study the movement of the ventricle wall directly.
In the long term, the team’s findings might enable the development of new treatments for lesions. Ordinarily, pharmaceutical treatments struggle to cross the blood-brain barrier and reach affected areas, but the new research suggests that it might be possible to channel drugs to lesions directly through leaks in the ventricular wall. “That’s still a long way off, and we didn’t study it directly,” Weickenmeier cautioned. “But it’s an intriguing possibility.”
The broader takeaway from the team’s research, explained Weickenmeier, is that the brain’s aging process is mediated by physical processes, including the pressure of circulating blood and CSF. That underscores the need for healthy behaviors — such as getting enough exercise and avoiding harmful substances — that can reduce those strains on the brain.
Story Source:
Materials provided by Stevens Institute of Technology. Note: Content may be edited for style and length.