
Covid Vaccinations Do Not Lead to Pre-term Births, Study Says

Women who received Covid vaccinations while pregnant were at no greater risk of delivering their babies prematurely or of giving birth to unusually small babies than pregnant women who did not get vaccinated, a new study reports.The study, one of the first to examine the health of babies born to women vaccinated during pregnancy, was a reassuring signal. Low-birth-weight babies and infants born early are more likely to experience developmental delays and other health problems.An earlier study had found that women vaccinated during pregnancy did not face a higher risk of miscarriage than the unvaccinated.The new study looked at some 46,079 singleton pregnancies that resulted in a live birth, including some 10,064 among women who received one or more doses of Covid vaccine between Dec. 15, 2020, and July 22, 2021, during their pregnancies. Most had received the vaccines made by Pfizer-BioNTech or Moderna, and the vast majority were inoculated during their second or third trimester.Overall, 6.6 percent of the babies were born prematurely, before 37 weeks of pregnancy, and 8.2 percent were born small for their gestational age, weighing less than 5 pounds and 8 ounces. Researchers found no difference in the rates among mothers who had been vaccinated while pregnant and those who had not.“We plan to do follow-up studies on infants and their development, but there hasn’t been enough time to do them yet,” said Dr. Heather S. Lipkind, a maternal fetal medicine specialist at Yale University and lead author on the new research.The study was conducted by the Centers for Disease Control and Prevention, in collaboration with Dr. Lipkind, HealthPartners Institute, Kaiser Permanente researchers and the Harvard Pilgrim Health Care Institute. The risks of pre-term birth, which appear to be higher when pregnant women are infected with the coronavirus, are well established, she said: “With each week of gestation, the brain develops more. If you have Covid and have to deliver preterm, that can also affect long-term development.”Another benefit to vaccination is that women may pass on coronavirus antibodies to their infants, helping to protect them from illness, Dr. Lipkind added.Pregnant women who become infected face a higher risk of developing severe disease, and federal health officials have implored them to get vaccinated. Nevertheless, vaccination rates remain low among pregnant women — about 31 percent as of late September.Vaccination rates also vary widely by community. While almost half of all pregnant Asian Americans are vaccinated, only 25 percent of pregnant Hispanic women are, and only 15 percent of pregnant Black women, according to the C.D.C.“I can tell you, anecdotally, that in my practice women who are not vaccinated are for sure getting way sicker,” Dr. Lipkind said, “and we’re seeing pre-term birth in pregnant women who had Covid and loss of pregnancy. It’s very, very tragic.”She strongly encourages her patients to get vaccinated, especially now that the highly contagious Omicron variant is circulating. But she often faces fierce resistance, she said.“I think people are just afraid of the unknown in general with pregnancy,” Dr. Lipkind said. “This new research should make people feel a little better about vaccination.”
Read more →Pregnancy: Mum felt 'fat-shamed' by health staff

A mum-of-four has said she felt she was “fat-shamed” by hospital staff during her pregnancy scan. Alexandra Dodds said jokes were made about her weight such as “hope you’ve stopped having your Christmas snacks”.”I think it was just like banter, but I feel you can’t banter about that,” she said. Studies have found women with a higher BMI during pregnancy feel “deeply stigmatised”.The Royal College of Midwives (RCM) said care should be based on respect and understanding of women’s needs.
Read more →U.S. Doubles Paxlovid Covid Pill Order

The United States government doubled its order for Pfizer’s Covid pills on Tuesday, a move that will modestly increase the nation’s very limited supplies of the treatment in the short term, as the country deals with a record-setting surge in coronavirus cases.The new order will eventually provide enough pills for 10 million Americans, bringing the government’s total order of the drug to 20 million treatment courses. But they will not all be available right away. Only 35,000 of the additional courses would be delivered this month, and 50,000 more in February, to add to the 350,000 treatment courses that were already expected in the next two months, according to a senior administration official.“We may need even more,” President Biden said on Tuesday, announcing the move ahead of a briefing he was set to receive from health advisers. “That’s the estimate we need right now.”The government has agreed to pay Pfizer $530 for each treatment course, the same amount it paid for its initial order late last year, the official said.The increase in supplies is likely to come as welcome news at a time when Pfizer’s pills and other Covid treatments are hard to find and demand for them is high. But monthly deliveries of the Pfizer treatment, known as Paxlovid, are not expected to ramp up into the millions until April, much too late to help with the current surge. The combined order is not due to be completely filled until the end of September.Still, Mr. Biden hailed the order as key component of the federal government’s winter pandemic response. “They’re a game-changer,” he said, “and have the potential to dramatically alter” the course of the pandemic.Paxlovid was authorized two weeks ago for use in high-risk Covid patients age 12 or older. The treatment, meant to be taken soon after the start of symptoms, has proved in clinical trials to be highly effective in staving off severe illness.But public health experts have warned that without adequate testing supply — a problem in many parts of the country — it could be difficult to quickly get the pill to those most in need.Mr. Biden on Tuesday said that the administration’s plan to have insurers reimburse people for at-home tests would go into effect soon, as would a website allowing Americans to order free tests delivered to their homes.“I know this remains frustrating,” he said. “Believe me, it’s frustrating to me. But we’re making improvements.”The first supplies of Paxlovid have already begun arriving in some parts of the country, but they are so limited in quantity that state health officials are recommending that they be used only for the highest-risk of high-risk patients.Arizona, for instance, advised that Paxlovid be given only to people over 70 who also have severe health conditions like end-stage heart disease, or to younger patients with weakened immune systems.State officials say they are carefully distributing the pills they have received to people most in need.In West Virginia, health officials have shipped around 20 treatment courses to each of 14 locations and reserved about 20 more in a central state repository for use in case of an outbreak, said Dr. Clay Marsh, the state’s Covid-19 czar.For the first few weeks of the rollout, he said, Paxlovid was sent to sites where people can also get tested for the virus, like primary-care doctors’ offices and drugstores, in an effort to “reduce the complexity and number of different touch points that people will have to make.”In Louisiana, health officials met last week with hospital executives from across the state, who pitched a plan the state adopted this week in its most recent allocation of 342 Paxlovid courses: sending the pill to hospital outpatient pharmacies.Dr. Joseph Kanter, Louisiana’s top health official, said the idea was to ease the strain on overflowing emergency departments and intensive care units, where physicians can prescribe the pill to patients at risk and discharge them before an infection spirals.That will shorten the time between when a patient is identified as a candidate for Paxlovid and when it is prescribed and taken, Dr. Kanter said.“There’s a limit to how much you can triage this from a top-down level,” he said. “You have to put it in the hands of providers and pharmacists and provide the best guidance you can, then step back and hope it gets to people who most need it.”
Read more →5 Tips for Spotting Melanoma and Other Skin Cancers
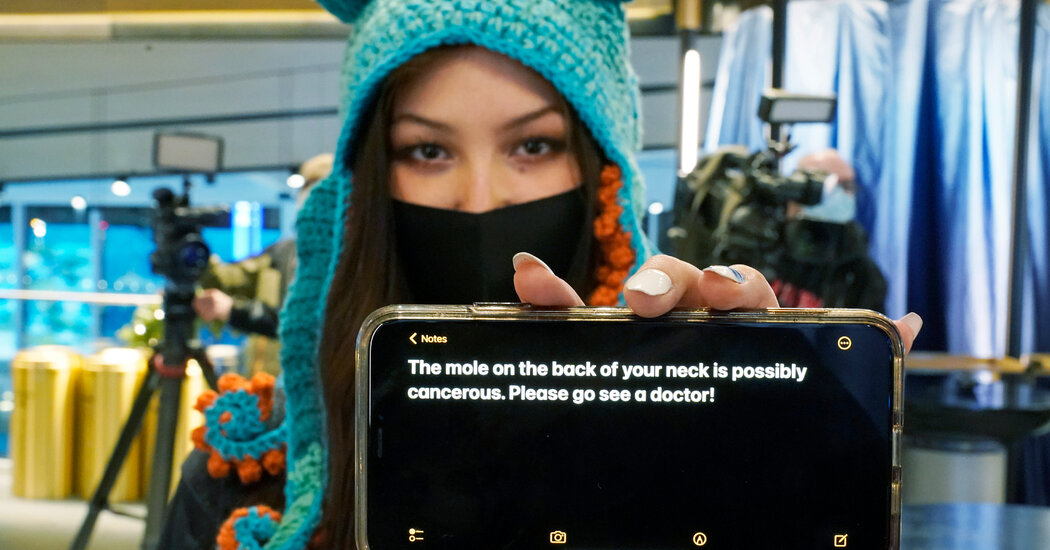
An unusual incident at a hockey game may have been lifesaving for one staff member with a suspicious skin mole.In October, Nadia Popovici, a Seattle Kraken hockey fan, went to a game with her parents. She spotted a strange-looking mole on the neck of an assistant equipment manager for the opposing team, the Vancouver Canucks, and typed out a message to him on her phone.“The mole on the back of your neck is possibly cancerous. Please go see a doctor!” the message read, with the words “mole,” “cancer” and “doctor” colored bright red.Her message may have saved his life. It turned out to be a melanoma, a particularly deadly type of skin cancer that, because it was detected early, could be removed before it had spread.“She took me out of a slow fire,” the assistant manager, Brian Hamilton, said at a recent news conference.Skin cancer is common, but often survivable. Basal and squamous cell carcinomas, by far the most common types of skin cancer, can be extraordinarily disfiguring but are rarely fatal.Melanoma is a different story. It accounts for just about 1 percent of all diagnosed skin cancers, but causes the vast majority of deaths. In 2021, the American Cancer Society estimated that doctors would diagnose about 106,110 new melanomas in the United States, and that about 7,180 people would die of the disease. The risk increases with age.Early detection can lead to effective treatment. The five-year survival rate for “thin melanoma,” Stage 1, when the cancer is less than one millimeter thick, is 99 percent, according to the American Cancer Society. Once it has spread to distant organs, Stage 4, the survival drops to 27 percent.“If you miss the beginnings of this one, you might actually miss the opportunity to save the person’s life,” said Dr. Allan C. Halpern, the chief of dermatology service at Memorial Sloan Kettering Cancer Center.So in light of the hockey “miracle” — and the new year — consider this your guide to setting some healthy skin care habits for 2022.1. Above all, look for … weirdIf you see something on your skin that is new, changing, not healing or doesn’t seem right, get it checked out by a doctor as soon as possible.“What we often refer to is the ‘ugly duckling sign,’” Dr. Halpern, a vice president of the Skin Cancer Foundation, said. “If it just looks different than everything else, get it checked out.”The Skin Cancer Foundation, founded in 1979, has long recommended an “ABCDE” test for worrisome lesions. It is a mnemonic device to check what to look for: A for asymmetry, when one half doesn’t match the other; B for an irregular border; C for colors that might be different from one another; D for a large diameter, or anything approaching the size of a Cheerio or a pencil eraser; and E for evolving, meaning that it changes over time.Those recommendations are still useful, but they may be somewhat limiting. “Many melanomas and most nonmelanoma skin cancers don’t fall under the ABCDE pattern,” the foundation reported in its journal in 2019. “When we educate people about the warning signs of skin cancer, we often hear from them, ‘Mine didn’t look like that.’”Many dermatologists recommend people look for things that feel out of the ordinary. Is it new? Is it growing? Is it refusing to heal? Those may all be indications that it’s time to see a doctor.Dr. Halpern said to look for any unusual lesions that make you anxious. “People have a sense of normal,” he said. “It’s really important not to downplay people’s visceral knowledge of normal versus out of the ordinary.”2. Set a regular scan reminderYou won’t know what’s weird if you don’t carve out time to look. The Cleveland Clinic recommends a monthly scan, though some doctors say you can opt for a quarterly skin check instead.“If you don’t examine yourself at least once a month, you don’t have a good mental memory of what you look like, so you won’t be able to spot change,” Dr. Halpern said.To scan, stand in front of a full-length mirror; have a hand mirror on deck for hard-to-reach places. Start systematically, from the top of your head down. Don’t forget your scalp and neck, or under the nails. The Skin Cancer Foundation has a guide, and the American Academy of Dermatology Association has a video tutorial.And remember, look for weird. If there’s a mole that you think looks out of the ordinary, get it checked out. You can also take pictures of your moles so you can compare them on your next scan. If you’re noticing changes, or if you develop a sore that does not heal, call a dermatologist.3. Do it with a buddyA recent study found that married people are more likely than the unmarried to get timely diagnosis and treatment for malignant skin cancer. That may be because they have someone else who sees them almost every day, and who might notice something unusual. Spouses may also urge their partner to visit a doctor.“The number of times that I’ll see someone at the office who comes in and either they, or their significant other, has said: ‘That’s not just like it was on you before. I can’t say why it is, but it’s just different,’” said Dr. Aaron Mangold, the divisional chair of clinical dermatology at the Mayo Clinic.If you live alone, a buddy system might work. Consider setting up a monthly reminder with a roommate or a regular “mole check” evening with a close friend.4. Know your risk factorsYour skin, and your personal history, affect how often you have to check. If you’re at high risk of skin cancer, you should have a different relationship to your dermatologist and your moles.People who have a family history of melanoma are more likely to develop the disease. “If you’ve gotten a lot of blistering sunburns, maybe five by the time you’re 18,” or used a tanning bed, you are at increased risk, Dr. Deborah S. Sarnoff, the president of the Skin Cancer Foundation, said. “That really bumps it up, the way smoking bumps up lung cancer.”Your skin color plays a role, too. People with light skin, blond or red hair, blue eyes, or many freckles and moles are more prone to developing skin cancer than people of color — it’s more than 20 percent more common in white people than Black people, according to the American Cancer Society. That’s because most skin cancers are sun related, and darker skin is less at risk for sun-induced cancers.In people of all races, however, skin cancers can also present in places that do not regularly get sun exposure, like the hands or soles of their feet, the mucous membranes (gums, lips) and the nail beds. These cancers may be more deadly, because they are often diagnosed at a later stage. And although melanoma is more common when you’re older, young people can get skin cancer, too. In fact, it is one of the most common cancers in people younger than 30, especially young women. The Cleveland Clinic says you should “always be suspicious of a new mole that develops after the age of 30.” Many are harmless, but it’s good to check with a dermatologist, just to be safe.5. If you think you have reason to be worried, see a dermatologistCome to the doctor’s appointment prepared to point out any unusual spots you’ve noticed, and to have your entire body checked. “It is every square centimeter of skin,” said Dr. Ashwani Rajput, the director of the Johns Hopkins Kimmel Cancer Center for the Washington, D.C., region, who treats patients with melanoma.The Skin Cancer Foundation recommends you remove makeup before your exam, if you wear any, so it will be easier to spot suspicious moles.“Leave any embarrassment at the door,” Dr. Sarnoff said, adding, “You’re there to have your skin looked at.”A screening can take up to 30 minutes. A doctor who finds a mole that might be cancerous will often numb the area and then remove some or all of it for a biopsy. The doctor will share the results and discuss next steps with you if the biopsy returns a positive cancer result.“The overwhelming majority of these visits do end up being covered by insurance,” Dr. Halpern said, especially if you are at high risk or there is cause for concern.
Read more →Custom finger clip offers a new way to measure blood pressure, other vitals

Monitoring a person’s blood pressure on a regular basis can help health care professionals with early detection of various health problems such as high blood pressure, which has no warning signs or symptoms. However, many things can alter an accurate blood pressure reading, including a patient’s nervousness about having their blood pressure taken at a doctor’s office, otherwise known as “white coat syndrome.”
Now, researchers at the University of Missouri are customizing a commercial finger clip device to provide a rapid, noninvasive way for measuring and continually monitoring blood pressure. The device can also simultaneously measure four additional vital signs — heart rate, blood oxygen saturation, body temperature and respiratory rate, said Richard Byfield, a mechanical and aerospace engineering graduate student in the MU College of Engineering, and the lead author on the study.
“Typically, calculating someone’s blood pressure at a hospital or clinic involves using an inflatable cuff wrapped around their arm, but there are three issues with that method — it can cause damage to someone’s arteries if done repeatedly within a short amount of time; people’s blood pressure can rise due to nervousness; and it can take up to 30 seconds to complete,” Byfield said. “Our device can record someone’s blood pressure within five seconds by using optical sensors placed on the fingertip that measure the amount of light reflected off the blood vessels underneath the surface of the skin.”
This process is called photoplethysmography (PPG), and the device uses two PPG sensors located at two different points on a finger to capture someone’s pulse in order to calculate pulse wave velocity, or how fast the blood is traveling through the bloodstream. Once the data from the pulse wave velocity is gathered, it’s transmitted wirelessly to a computer for signal processing and blood pressure calculation by a machine learning algorithm. The researchers said other studies have also shown pulse wave velocity has a strong correlation with blood pressure.
An early test of the device with 26 study participants has provided an accuracy rate of about 90% for systolic blood pressure, and a 63% accuracy rate for diastolic blood pressure. Byfield said the accuracy rate differs between systolic and diastolic because diastolic, which is a person’s minimum blood pressure, can change significantly depending on a person’s age, and can also be controlled by various factors, including age, artery stiffness, overall health and body weight.
Byfield and his colleagues also acknowledge there are some issues with making PPG sensors work to obtain these measurements.
“Typically, there are a few problems with PPG sensors,” Byfield said. “One is called artifact motion — if you move a PPG sensor while it’s reading, it can affect the waves that are being recorded. On top of that, we found that differences in pressure can alter the waves, but with a finger clip design, a spring provides constant pressure. Another reason this method hasn’t been explored much before is typically these finger clips only have one sensor, but we have two sensors in our device.”
A provisional patent has been filed for the device. Researchers are currently working on developing the device for at-home use, and their long-term goal includes potential clinical and commercial applications. Byfield said a clinical application could help relieve some burdens for nurses who deal with multiple devices to monitor a patient’s vital signs.
Researchers are also working to incorporate the device in data collection for future studies by developing predictive computational models to help identify vital signs that could serve as indicators for multiple human diseases, including COVID-19 and the flu, said Jian Lin, William R. Kimel Faculty Fellow and associate professor of mechanical and aerospace engineering.
“Our goal is to develop a broader impact for our device beyond a new way to measure vital signs,” said Lin, who is the corresponding author on the study.
Story Source:
Materials provided by University of Missouri-Columbia. Note: Content may be edited for style and length.
One autoimmune disease could lead to another
Researchers at the University of Colorado Anschutz Medical Campus have discovered that having one kind of autoimmune disease can lead to another.
The scientists serendipitously found that mice with antibody-induced rheumatoid arthritis in their joints went on to develop spinal lesions similar to those in axial spondyloarthritis (AxSpA) which causes fusion of the vertebrate and curvature, or bending, of the backbone.
The study was published today in the journal Immune Network.
“Our results suggest that one autoimmune disease, such as inflammatory arthritis, may also lead to a secondary autoimmune disease such as AxSpA,” said the study’s lead author Nirmal Banda, PhD, professor in the division of rheumatology at the University of Colorado School of Medicine. “This interesting disease association may be due to the binding of anti-collagen autoantibodies to the spine, or to some alteration of the immune system that requires further investigation.”
These same anti-collagen antibodies are also present in humans with arthritis. They directly attack joint cartilage resulting in inflammation and pain.
Banda noted that every mouse injected with collagen antibody-induced arthritis (CAIA) developed arthritis and then curvature of the spine consistent with axial spondyloarthritis.
New gene therapy approach offers a potential long-term treatment for limb-girdle muscular dystrophy 2B
Children’s National Hospital experts developed a new pre-clinical gene therapy for a rare disorder, known as limb-girdle muscular dystrophy (LGMD) 2B, that addresses the primary cellular deficit associated with this disease. Using a single injection of a low dose gene therapy vector, researchers restored the ability of injured muscle fibers to repair in a way that reduced muscle degeneration and enhanced the functioning of the diseased muscle. The treatment was safe, attenuated fibro-fatty muscle degeneration, and restored myofiber size and muscle strength, according to the study published in the Journal of Clinical Investigation.
With an incidence of less than 1 in 100,000, LGMD2B is a rare disorder caused by a genetic mutation in a large gene called dysferlin. This faulty gene leads to muscle weakness in the arms, legs, shoulder and pelvic girdle. Affected children and adults face trouble walking, climbing stairs, and getting out of chairs. Individuals typically lose the ability to walk within years after the onset of symptoms, and often need assistance with everyday tasks such as showering, dressing and transferring.
This study described a new approach that avoids the need for packaging a large gene, like dysferlin, or giving a large vector dose to target the muscles, which are bottlenecks faced in ongoing gene therapy efforts aimed at muscular dystrophies.
“Currently, patients with LGMD2B have no gene or drug-based therapies available to them, and we are amongst the few centers developing therapeutic approaches for this disease,” said Jyoti K. Jaiswal, M.Sc. Ph.D., senior investigator of the Center for Genetic Medicine Research at Children’s National. “We are working to further enhance the efficacy of this approach and perform a longer-term safety and efficacy study to enable the clinical translation of this therapy.”
The genetic defect in dysferlin that is associated with LGMD2B causes the encoded protein to be truncated or degraded. This hinders the muscle fiber’s ability to heal, which is required for healthy muscles. In recessive genetic disorders, like LGMD2B, common pre-clinical gene therapy approaches usually target the mutated gene in the muscle, making them capable of producing the missing proteins.
“The large size of the gene mutated in this disease, and impediments in body-wide delivery of gene therapy vectors to reach all the muscles, pose significant challenges for developing gene therapies to treat this disease,” said Jaiswal.
To overcome these challenges, the researchers found another way to slow down the disease’s progression. The authors built upon their previous discovery that acid sphingomyelinase (hASM) protein is required to repair injured muscle cells. In this current work, the research team administered a single in vivo dose of an Adeno-associated virus (AAV) vector that produces a secreted version of hASM in the liver, which then was delivered to the muscles via blood circulation at a level determined to be efficacious in repairing LGMD2B patient’s injured muscle cells.
“Increased muscle degeneration necessitates greater muscle regeneration, and we found that improved repair of dysferlin-deficient myofibers by hASM-AAV reduces the need for regeneration, causing a 2-fold decrease in the number of regenerated myofibers,” said Daniel Bittel, D.P.T., PhD., research postdoctoral fellow of the Center for Genetic Medicine Research at Children’s National and a lead author of this study.
Sreetama Sen Chandra, Ph.D., who was a research postdoctoral fellow at Children’s National at the time of this study and served as co-lead author, also added that “these findings are also of interest to patients with Niemann-Pick disease type A since the pre-clinical model for this disease also manifests poor sarcolemma repair.”
Children’s National researchers of the Center for Genetic Medicine Research and the Rare Disease Institute (RDI) are constantly pursuing high-impact opportunities in pediatric genomic and precision medicine. Both centers combine its strengths with public and private partners, including industry, universities, federal agencies, start-up companies and academic medical centers. They also serve as an international referral site for rare disorders.
Roundworm linked to lower lung-function and asthma in younger males
By looking at the exposure to the parasitic roundworm Ascaris lumbricoides/suum in Nothern Europe (Norway, Denmark and Estonia), the study finds that younger men exposed to Ascaris had a striking reduction in lung function and nearly five times higher odds of having asthma compared to the non-exposed. These effects were independent of smoking and other exposures such as house dust mites.
The paper “Ascaris exposure associated with lung function, asthma and DNA-methylation in Northern-Europe” was just published in The Journal of Allergy and Clinical Immunology.
The study is a collaboration between the University of Bergen, Tartu University Hospital Lung Clinic, University of Aarhus, the University of Birmingham and the University of Cape Town.
Differences in gender
A curious finding in the study was that among women, lung function was not significantly lower in the Ascaris seropositive. In fact, the seropositive appeared to have even less asthma than the rest. This is the first research of its kind to show substantial gender differences in terms of helminth (parasitic worms) exposures and subsequent outcomes in humans.
The researchers also found that Ascaris infection in Europe might be an overlooked risk factor for asthma and respiratory health.
May result in lung damage
It has previously been assumed that infections of roundworms have not been of significance in Europe, but the new findings indicate that exposure could potentially be a lot more common than assumed. For persons affected, this may result in serious lung damage with the risk of having a long-term impairment of lung function
Parasitic worm-infections are normally considered to be a problem only in low and middle-income countries. These findings present them as being of much greater importance in Europe.
This is also the first study to report a connection between reduced lung function and Ascaris exposure, according to the researchers.
Story Source:
Materials provided by The University of Bergen. Note: Content may be edited for style and length.
New route for regulating blood sugar levels independent of insulin
The discovery of insulin 100 years ago opened a door that would lead to life and hope for millions of people with diabetes. Ever since then, insulin, produced in the pancreas, has been considered the primary means of treating conditions characterized by high blood sugar (glucose), such as diabetes. Now, Salk scientists have discovered a second molecule, produced in fat tissue, that, like insulin, also potently and rapidly regulates blood glucose. Their finding could lead to the development of new therapies for treating diabetes, and also lays the foundation for promising new avenues in metabolism research.
The study, which was published in Cell Metabolism on January 4, 2022, shows that a hormone called FGF1 regulates blood glucose by inhibiting fat breakdown (lipolysis). Like insulin, FGF1 controls blood glucose by inhibiting lipolysis, but the two hormones do so in different ways. Importantly, this difference could enable FGF1 to be used to safely and successfully lower blood glucose in people who suffer from insulin resistance.
“Finding a second hormone that suppresses lipolysis and lowers glucose is a scientific breakthrough,” says co-senior author and Professor Ronald Evans, holder of the March of Dimes Chair in Molecular and Developmental Biology. “We have identified a new player in regulating fat lipolysis that will help us understand how energy stores are managed in the body.”
When we eat, energy-rich fats and glucose enter the bloodstream. Insulin normally shuttles these nutrients to cells in muscles and fat tissue, where they are either used immediately or stored for later use. In people with insulin resistance, glucose is not efficiently removed from the blood, and higher lipolysis increases the fatty acid levels. These extra fatty acids accelerate glucose production from the liver, compounding the already high glucose levels. Moreover, fatty acids accumulate in organs, exacerbating the insulin resistance — characteristics of diabetes and obesity.
Previously, the lab showed that injecting FGF1 dramatically lowered blood glucose in mice and that chronic FGF1 treatment relieved insulin resistance. But how it worked remained a mystery.
In the current work, the team investigated the mechanisms behind these phenomena and how they were linked. First, they showed that FGF1 suppresses lipolysis, as insulin does. Then they showed that FGF1 regulates the production of glucose in the liver, as insulin does. These similarities led the group to wonder if FGF1 and insulin use the same signaling (communication) pathways to regulate blood glucose.
It was already known that insulin suppresses lipolysis through PDE3B, an enzyme that initiates a signaling pathway, so the team tested a full array of similar enzymes, with PDE3B at the top of their list. They were surprised to find that FGF1 uses a different pathway — PDE4.
“This mechanism is basically a second loop, with all the advantages of a parallel pathway. In insulin resistance, insulin signaling is impaired. However, with a different signaling cascade, if one is not working, the other can. That way you still have the control of lipolysis and blood glucose regulation,” says first author Gencer Sancar, a postdoctoral researcher in the Evans lab.
Finding the PDE4 pathway opens new opportunities for drug discovery and basic research focused on high blood glucose (hyperglycemia) and insulin resistance. The scientists are eager to investigate the possibility of modifying FGF1 to improve PDE4 activity. Another route is targeting multiple points in the signaling pathway before PDE4 is activated.
“The unique ability of FGF1 to induce sustained glucose lowering in insulin-resistant diabetic mice is a promising therapeutic route for diabetic patients. We hope that understanding this pathway will lead to better treatments for diabetic patients,” says co-senior author Michael Downes, a senior staff scientist in the Evans lab. “Now that we’ve got a new pathway, we can figure out its role in energy homeostasis in the body and how to manipulate it.”
Other authors included Sihao Liu, Emanuel Gasser, Jacqueline G. Alvarez, Christopher Moutos, Kyeongkyu Kim, Yuhao Wang, Timothy F. Huddy, Brittany Ross, Yang Dai, David Zepeda, Brett Collins, Emma Tilley, Matthew J. Kolar, Ruth T. Yu, Annette R. Atkins and Alan Saghatelian of Salk; Tim van Zutphen, Theo H. van Dijk and Johan W. Jonker of the University of Groningen, in the Netherlands.
The research was supported by the National Institutes of Health, the Nomis Foundation, the March of Dimes, Deutsche Forschungsgemeinschaft (DFG), Netherlands Organization for Scientific Research, the European Foundation for the Study of Diabetes and the Swiss National Science Foundation.