
New studies point the way to broadly effective treatments for ALS

Each year in the U.S., 5,000 patients receive a diagnosis of ALS, an incurable neurodegenerative disease that will likely kill them within two to five years. In the quest to find a cure for these patients, a team of researchers led by USC Stem Cell scientist Justin Ichida has identified two promising avenues for developing new treatments for diverse forms of this devastating disease, which is also known as amyotrophic lateral sclerosis or Lou Gehrig’s disease. Their findings are published in a pair of studies: the first appearing in the journal Cell Stem Cell on February 2, and the second in the journal Cell on February 7.
“A minority of patients have a variety of genetic causes of ALS that can be inherited within families, and a majority have what is known as “sporadic” disease because its causes are unknown,” said Gabriel Linares, a postdoc in the Ichida lab and a co-first author on both studies. “This makes it a difficult challenge to find one treatment that will work for all patients with ALS.”
To meet this challenge, the researchers collected skin or blood samples from patients with both familial and sporadic ALS. The scientists reprogrammed the skin and blood cells into motor neurons, which are the nerve cells responsible for movement that degenerate in the disease. These patient-derived motor neurons provided an opportunity to screen thousands of FDA-approved drugs and drug-like molecules to find ones that might be effective against multiple forms of ALS.
In the Cell Stem Cell study, co-first authors Linares and Yichen Li found that several of the most effective drugs and drug-like molecules increased the activity of androgens, the well-known group of sex hormones that include testosterone. However, because androgen-boosting drugs could have undesirable or unsafe side effects for patients with ALS, the scientists aimed to identify a genetic change that might yield similar results.
To accomplish this, they leveraged a public bioinformatics database known as Connectivity Map, developed by the Broad Institute of Harvard and MIT. By analyzing this vast database of information about how drugs affect the genetic landscape underpinning diseases, the scientists accurately predicted that suppressing the SYF2 gene would increase the survival of motor neurons derived from patients with diverse forms of ALS. In addition, suppressing this gene reduced neurodegeneration, motor dysfunction, and other symptoms in mice with ALS.
“What’s really exciting is that SYF2 suppression improved symptoms and pathology related to a protein called TDP-43, which can become toxic and is implicated in close to 97 percent of cases of ALS,” said Li, a postdoc in the Ichida Lab.
In the second study published in Cell, co-first authors Shu-Ting (Michelle) Hung and Linares detail how inhibiting a protein, the PIKFYVE kinase, could represent another effective strategy for treating many different forms of ALS.
In an extensive series of experiments, the researchers inhibited PIKFYVE using the drug apilimod, as well as through genetic and RNA-based approaches, in fruit flies, roundworms, mice, and motor neurons derived from patients with different forms of ALS.
They found that inhibiting PIKFYVE reduced neurodegeneration, improved motor function, and lengthened life by stimulating motor neurons to clear toxic proteins through a process of exocytosis, in which membrane-bound sacs envelop and actively transport waste to the exterior of the cell.
“We were able to pinpoint precisely how PIKFYVE inhibition mitigates neurodegeneration, which is important for informing the development of new targeted treatments,” said Hung, a PhD student in the Ichida Lab.
Ichida, who is the John Douglas French Alzheimer’s Foundation Associate Professor of Stem Cell Biology and Regenerative Medicine at USC, and a New York Stem Cell Foundation-Robertson Investigator, added “Our discoveries bring us closer to achieving our big picture goal: finding treatments that can be broadly effective for all patients who suffer from ALS.”
Additional co-authors on both studies are: Yunsun Eoh, Manuel Santana, Jonathan Chang, and Joscany Perez from USC; and Wen-Hsuan Chang, Stacee Mendonca, Sarah Hong, and Samuel V. Alworth from AcuraStem, Inc.
For the Cell Stem Cell study, co-authors also include Hung, Jasper Rubin-Sigler, Wenxuan Guo, Yi-Hsuan Huang, Nomongo Dorjsuren, Michael Chickering, Hao-Jen Deng, Kieu-Tram Bach, and Kamden Gray from USC; Johnny Yu and Hani Goodarzi from the University of California, San Francisco; Tze-Yuan Cheng, Chi Chou Huang, and James Lee from Leica Microsystems; and Jeffrey Rosenfeld from Loma Linda University.
For the Cell study, additional co-authors include Li, Yingxiao Shi, Sarah Perry, Alexander Couto, Jesse Lai, Eric Hendricks, Yaoming Wang, Berislav V. Zlokovic, and Dion K. Dickman from USC; Gopinath Krishnanand Fen-Biao Gao from the University of Massachusetts; Chuol Kueth, Samantha Macklin-Isquierdo, and Daniela C. Zarnescu from Penn State University; and Sarah Duhaime, Claudia Maios, and J. Alex Parker from the Université de Montréal.
Frequent Blood Pressure Monitoring Is Needed During and After Pregnancy

The U.S. Preventive Services Task Force warned of a rise in hypertensive disorders among pregnant women, particularly women of color.Health care providers must check pregnant patients’ blood pressure regularly, starting early in pregnancy and continuing for at least six weeks after childbirth, according to new draft recommendations from the U.S. Preventive Services Task Force.The task force issued the draft recommendations on Tuesday amid growing concern about a rise in maternal mortality. Pregnancy-related deaths in the United States are the highest among industrialized nations, and hypertensive disorders of pregnancy are among the leading causes.Blood pressure disorders in pregnancy have doubled in prevalence in the past three decades, affecting one in 10 pregnancies now, up from one in 20 in 1993. They are a leading cause of death during and after pregnancy among Native American women and the leading cause of death among Black women.The groups face maternal mortality rates that are up to three times as high as those among white women. The disorders pose a high risk of stroke to Black and Hispanic women, the task force noted. Yet women of color were underrepresented in most clinical trials that tested screening regimens for the condition.The task force called on health care providers to offer better support for pregnant women of color, and for physicians to be aware of their increased risks so they can “focus clinical energy and resources to those most likely to suffer morbidity or mortality.”“Our moms are dying,” Dr. Wanda Nicholson, vice chair of the task force, said, adding that the new draft recommendations aimed “to call attention to the racial disparities in maternal deaths and morbidity.”The recommendations call for more research into the conditions, and they urge doctors and midwives to use standard, evidence-based treatment for all patients. Not all pregnant women who are affected receive the recommended care for blood pressure disorders, though Black women are more likely to get appropriate care than white women.“The take-home point is that we know, unequivocally, that consistent checking of blood pressure during pregnancy makes a difference for our moms and babies,” said Dr. Nicholson, a senior associate dean for diversity, equity and inclusion at the Milken Institute School of Public Health at George Washington University.The onset of a severe blood pressure condition called pre-eclampsia/eclampsia often occurs after the first 20 weeks of pregnancy. Low-dose aspirin starting at 12 weeks gestation is recommended for women at heightened risk — a large group that includes patients with pre-existing conditions like diabetes or lupus, those who are 35 and older or under the age of 15, patients who have undergone in vitro fertilization, and those pregnant for the first time.The report suggests all Black women who are pregnant and have at least one risk factor for pre-eclampsia/eclampsia should be put on low-dose aspirin, which may prevent or at least delay the development of the condition.Patients with high blood pressure during pregnancy must be monitored very closely, said Dr. Christian Pettker, a professor of obstetrics, gynecology and reproductive science at Yale School of Medicine and a co-author of treatment guidelines for the American College of Obstetricians and Gynecologists.“People who have elevated blood pressure in pregnancy are managed very differently than those who don’t,” Dr. Pettker said.Health care providers should prescribe medication for the blood pressure, and run additional blood tests and urine tests to check for abnormalities, as well as fetal ultrasounds to monitor the baby’s growth, Dr. Pettker said.In severe cases, the baby may be delivered early. Patients should report to their doctors symptoms including unusual headaches, sharp upper abdominal pain and blurry vision. The postpartum period is a critical one, as the risk of dying of a hypertensive disorder is highest then.Dr. Pettker warned that there may be a tendency among some health providers to dismiss high blood pressure readings in pregnant patients because they are generally young and healthy. But that is a mistake.“We sometimes try to normalize it — they look healthy, and seem to be doing great. But it might be an important signal,” Dr. Pettker said, adding that the medical community had “a lot of work to do to make sure that we take even mild blood pressure as a signal to pay attention to, and to pay attention in the same way for all the different people who present to us for prenatal care.”Blood pressure disorders have potentially serious long-term repercussions for the mother and the baby, and they are linked to preterm births and stillbirths, as well as to a long-term risk of heart disease in the mother.Hypertension can restrict fetal growth because it impedes blood flow, and can result in a medically induced preterm birth, because delivery of the baby resolves the disease and may be necessary to save the mother’s life and health.Women who had pre-eclampsia when they delivered are also at high risk of developing heart failure after childbirth, and Black women are at double the risk of white women, according to new findings by Truveta Research, the research arm of Truveta, a for-profit collective of health systems that uses de-identified patient data for research.Though the reasons for the disparity are not known, some may be caused by unequal access to care and by the failure of care givers to listen when women report unusual symptoms, Dr. Charlotte Baker, Truveta’s director of epidemiology, said. Dr. Baker lost a friend to the condition just months after the friend gave birth.“My friend had complained multiple times to her physicians, but they brushed her off,” she said.No one knows exactly why hypertensive disorders have doubled in prevalence in the past three decades, but women are having children at older ages than in the past. They are heavier than they used to be, as are all Americans, and a greater number have high blood pressure even before they become pregnant.Living conditions, known as social determinants of health, also play a role in maternal health, and recent studies have implicated housing instability and food insecurity in blood pressure disorders and other pregnancy complications. Disparities in access to health care services may also play a role.Maternal mortality rates in the United States have been rising in recent decades, and rose in 2021 to 1,178 deaths, up from 861 deaths in 2020, according to provisional figures in a recent Government Accountability Office report.
Read more →Kourtney Kardashian's Lemme vagina gummies? Don't bother, say experts

Published1 day agoShareclose panelShare pageCopy linkAbout sharingImage source, Getty ImagesBy Charlotte Simpson and Bonnie McLarenNewsbeat reportersShe might be one of the world’s most famous reality TV stars, but Kourtney Kardashian has had a bit of a career change.The 43-year-old has been gradually moving into the world of wellness with her blog, Poosh. And last year she launched a line of supplements called Lemme. But her latest addition to the vitamin range is raising some eyebrows, as she claims they can boost the health of your vagina. To promote the product – called Lemme Purr – she posted an Instagram video of herself, surrounded by cats, as she eats one of the gummies.”Vaginal health is such an important part of a woman’s overall wellbeing (and not talked about enough) which is why we are so excited to launch this,” the caption reads.One of the main claims Kourtney makes is that the vitamin sweets can alter the taste of the vagina.”Give your vagina the sweet treat it deserves (and turn it into a sweet treat),” Kourtney continues.’Grift’She says the product uses “pineapple and Vitamin C and probiotics to target vaginal health and pH levels that support freshness and taste”. Dr Jen Gunter, a gynaecologist and author of myth-busting bestseller The Vagina Bible, called Kourtney out on Instagram.”Anyone who suggests that your vagina isn’t fresh or needs an improved taste is a misogynist and awful person,” she wrote. “And yes that includes you @kourtneykardash and your @lemme grift.” Jen also disputes the belief that pineapples can affect the taste of your bodily fluids. UK chain Lloyd’s Pharmacy says it’s “normal for vaginas and vaginal fluids to have a slight smell, which will vary according to hormones, activity, hygiene and diet”.’See your GP, not a Kardashian’Maddy Dann, a 30-year-old A&E doctor, regularly speaks about sexual health on TikTok – and she’s told BBC Newsbeat why she doesn’t think the supplements will work.”Every person with a vulva or vagina is going to have a different odour, it’s going to have a different scent, a different taste and a different amount of discharge,” she says. “And so what this product suggests is that every woman needs to have the same tasting, the same smelling, vagina or discharge – and that’s just not realistic.”Maddy worries that the ad will give women the idea that something “entirely normal” is a problem that only the product can solve.She adds that the gummies “probably won’t be useful for most people” and that “there’s no such thing as an unclean vagina, the vagina self-cleans”.Get tested more, urges sexual health charityWhy TikTok has got us talking about mascaraFive things everyone with a vagina should know”While they make strong arguments with all these buzzwords, like vaginal pH and microbiome, in a healthy person probiotics and supplements aren’t always recommended unless there’s a confirmed deficiency in whatever you’re supplementing,” she adds.But Maddy’s top piece of advice? “If your odour or your discharge changes, you need to see a GP or a gynaecologist – not a Kardashian.”Newsbeat has contacted Kourtney Kardashian for comment. An FAQ on Lemme’s Instagram page says the brand uses “effective ingredients” that have been “clinically studied”.Follow Newsbeat on Twitter and YouTube.Listen to Newsbeat live at 12:45 and 17:45 weekdays – or listen back here.More on this storyKim K new owner of Princess Diana amethyst cross19 JanuaryAre silly TikTok life hacks secret fetish videos?29 December 2022
Read more →‘Miracle’ Cystic Fibrosis Drug Kept Out of Reach in Developing Countries
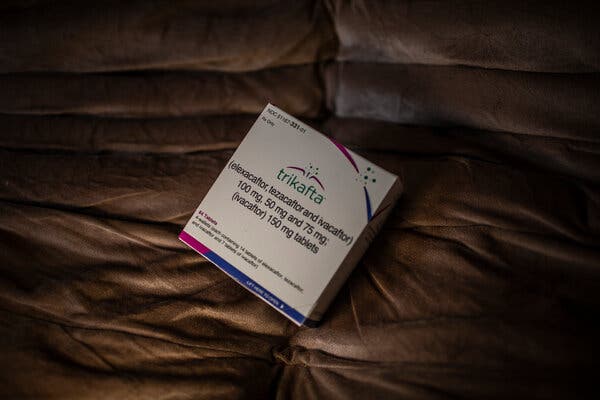
When Seshagiri Buddana learned of a powerful new cystic fibrosis drug that was transforming lives in the United States and Europe, he was filled with hope that it could help his son, Hemanth, who had spent much of his childhood in a hospital bed. But the family couldn’t get the drug because they live in India.The drug’s maker, Vertex Pharmaceuticals, a large biotech company based in Boston, is not making it available in India or virtually anywhere in the developing world. The company is not trying to sell it, or allowing a local company to make it. Vertex is blocking potential generic competitors by seeking patents in numerous countries.Hemanth died in December, a day before his ninth birthday and 18 months after he would have been eligible to get the drug, called Trikafta, had he lived in the United States.Throughout much of Asia, Africa and Latin America, families like Hemanth’s are watching Trikafta transform the lives of tens of thousands of cystic fibrosis patients in wealthy nations but say they are blocked by the company at every turn in their efforts to get the drug themselves.Trikafta, taken as three tablets a day, is the most powerful and widely used of Vertex’s four cystic fibrosis medications. With a list price of over $322,000 annually in the United States, it is expected to cost millions of dollars over the course of a patient’s lifetime. An analysis led by researchers in Britain found that a year’s supply of the drug could be manufactured at an estimated cost of just $5,700.Vertex has reported more than $15 billion in sales for Trikafta since it was first approved in 2019.This week, a group of patients and their families in four countries on four continents initiated legal and regulatory steps to try to force their governments to override intellectual property protections and allow a low-cost generic version of Trikafta to be imported or made locally. Under the process, known as compulsory licensing, generic makers would pay Vertex a royalty.Three of the actions are in India, Ukraine and South Africa — where Vertex has been obstructing efforts to make the drug available, patients and families say. The fourth is in Brazil, where Vertex is trying to win coverage for the drug; the patients and families’ concern there is that the brand-name drug will be too expensive.Trikafta is taken as three tablets a day and has a list price of $322,000 annually in the U.S.Dado Galdieri for The New York TimesRodrigo Rockenbach, 11, lives with cystic fibrosis in Brazil, where his father sued the government to get him Vertex’s drugs, and now helps other patients do the same.Dado Galdieri for The New York TimesRaphaelle Pereira of Brazil blows on a small pump as part of regular physiotherapy for her lungs.Dado Galdieri for The New York TimesCystic fibrosis is a genetic disease that damages the lungs and digestive system. Patients often die in early adulthood, but Trikafta is dramatically extending life expectancy.“Every patient in the world has access to the internet and wants this drug,” Christine Noke, a patient advocate in Turkey, said.More on IndiaAdani Group: Gautam Adani has often said his company’s goals were in lock step with India’s needs. Now, Adani Group’s fortunes are crashing, a collapse whose pain will be felt across the country.Gin Boom: A blossoming of gin distillers in the southern state of Goa is challenging India’s conservative attitude toward alcohol, along with the country’s often stultifying bureaucracy.On the Big Screen: A Mumbai theater has shown the movie “D.D.L.J.” nearly every day since 1995. In many ways, the India of today looks like the India on the screen.India’s Cram City: In Kota, students from across the country pay steep fees to be tutored for elite-college admissions exams — which most of them will fail.In theory, reaching patients in the developing world would bring in more revenue for a drug company. But some manufacturers resist making their drugs available in poorer countries at lower prices because doing so can erode their ability to charge more in high-income countries. Vertex, which has a monopoly on transformative cystic fibrosis drugs, said it was pushing to increase access globally.“Our teams are working every day to expand access to even more patients around the world through a range of routes, including in low-middle-income countries and low-income countries where access barriers are high due to challenging economic conditions and limited health care infrastructure,” Heather Nichols, a spokeswoman for Vertex, said.Ms. Nichols said that Vertex has begun a “product donation program” in low-income countries. She said the company has provided some form of access to at least one of its cystic fibrosis drugs in Brazil, Poland, Bulgaria, Estonia, Greece, Latvia, Slovakia, Slovenia, Romania and Oman. The company declined to specify which lower-resourced countries have access to Trikafta. The genetic defect that causes cystic fibrosis is most common in people of Northern European ancestry, as are the specific mutations needed for Trikafta to work. The number of cystic fibrosis patients in developing countries who are diagnosed and eligible for the drug is unknown but believed to number in the thousands.In India, a recent survey counted just 600 diagnosed cystic fibrosis patients. Counting India’s tens of thousands of patients who have not been diagnosed, some researchers estimate that India’s total cystic fibrosis population is higher than that in Europe. While a minority of Indians with cystic fibrosis are believed to have mutations that make them eligible for Trikafta, the size of India’s population translates into huge numbers of patients who could benefit from Trikafta.Hemanth Buddana, the Indian boy who died, was given therapies and antibiotics for his frequent lung infections, but there was little available in India to help him breathe or gain weight. Stuck in bed at home in Hyderabad, he taught himself to draw and to speak new languages. A genetic test confirmed that he would be eligible for Trikafta, which has a U.S. list price 20 times as much as the annual salary Mr. Buddana earns as an operations manager at Google. He joined other parents in pushing the Indian government to find a way to get Trikafta for their children. But there was no progress.Vihaan’s father, Sai, prepared his nebulizer at their home in Hyderabad, India.Atul Loke for The New York TimesA nearly abandoned oxygen cylinder in Ms. Pereira’s bedroom. She used a legal process to get Brazil’s public health system to supply her with Trikafta.Dado Galdieri for The New York TimesCheri Nel, 38, a South African who lives with cystic fibrosis, has launched a legal battle to make her government facilitate access to an affordable version of Trikafta.Joao Silva/The New York Times“They say it’s a miracle drug, but it’s not a miracle if it is not available to everyone who need it,” said Shwetha Sree, who also lives in Hyderabad. Her 5-year-old son, Vihaan, has cystic fibrosis — and the mutation that would make him eligible for the drug when he turns 6, if he were to live in the U.S. Since the fight over access to H.I.V. treatment in sub-Saharan Africa in the early 2000s, some drug companies have agreed to sell their medicines at a profitable but significantly lower price in developing countries. The companies also sometimes work with a drug importer to sell the products in those regions.There is also compassionate use, through which drug companies supply products to desperate patients in places where they are unauthorized. Vertex said that it has provided its medications free of charge to 6,500 patients worldwide that way. The company declined to say specifically where it has provided the drugs that way and where it is still doing so. A company can also agree to voluntary licenses, allowing generic manufacturers to make and sell a drug in certain countries, typically in exchange for a royalty. The Medicines Patent Pool, a United Nations-backed nonprofit that brokers that process by issuing sublicenses to generic manufacturers, said it has had no contact with Vertex.New drugs typically take longer to reach poorer countries. But frustration with Vertex’s failure to provide them with any form of access brought together cystic fibrosis patients online and led to a coordinated campaign for compulsory licensing.Governments are often reluctant to do compulsory licensing, which capital markets tend to view as an alarming crack in the wall of intellectual property protection. Still, even if governments refuse to issue a compulsory license, the patient actions may pressure Vertex to make Trikafta available in those countries.Cheri Nel, a 38-year-old investment banker in South Africa who has cystic fibrosis and is eligible for Trikafta, said that she had approached Vertex and suggested several ways the company could increase access and still safeguard its profit and intellectual property. She said she got nowhere and is now leading the action in South Africa.“There’s a balance: You want to keep companies incentivized to investigate and do research and development,” she said. “But it does them no financial harm to let us import a generic because they’re not even trying to sell it.”Vertex has not registered Trikafta with South Africa’s drug regulator, but the company said on Monday that it recently signed an agreement with a distributor there.Rodrigo Rockenbach, 11, uses a nebulizer to increase his intake of medication, as his parents look on.Dado Galdieri for The New York TimesRaphaelle Pereira of Brazil is looking forward to the removal of the port-a-cath that was inserted for her frequent infections and hospitalizations before she began treatment with Trikafta.Dado Galdieri for The New York TimesMs. Sree helped Vihaan with his physiotherapy after a session with the nebulizer.Atul Loke for The New York TimesIn many countries, Vertex has also been seeking patents which deter generic manufacturers from selling the drug there, according to patent filings viewed by The New York Times. The company has a running legal battle with Gador, one of several manufacturers in Argentina making lower-cost generic versions of Vertex’s drugs.Argentina does not recognize Vertex’s intellectual property rights because the company has not joined the global treaty on patent protection. Gador’s scientists reverse-engineered the Vertex drugs and began to sell them to Argentine patients. Then patients from foreign countries began to fly to Argentina to buy the drugs, which can cost as little as $18,000 per year using pesos exchanged on the black market. In the late 2010s, Gador tried to strike a deal with the Turkish government to import its low-cost version of another expensive Vertex cystic fibrosis drug, Orkambi. In 2018, Vertex sued Gador in a Turkish court, arguing that the company was infringing on Vertex’s patents. Vertex won, and the government abandoned the Gador deal.In 2021, after Trikafta had become available in parts of Europe, patients in Turkey began suing their government to try to get the drug.Today, more than 100 patients who have successfully sued the Turkish social security system are on Vertex medications, mostly Trikafta now. Dr. Bulent Karadag, the head of pediatric pulmonology at Turkey’s main cystic fibrosis center, said he had 250 more patients who have been confirmed as eligible for Trikafta but have not been able to get it. “Some patients say they can’t even afford the bus ticket to the hospital, let alone hire a lawyer,” he said. The U.S. list price for a year’s supply of Trikafta is nearly 60 times as much as the annual salary of a minimum wage earner in Turkey.Until Vertex’s drugs, patients had few options, mainly palliative treatment to help them breathe a bit better, and if they could get one, a lung transplant. Vertex’s drugs addressed the underlying cause of the illness, preventing patients’ lungs from clogging in sludgy mucus. Trikafta is stunningly effective at helping patients breathe better, keeping them out of the hospital and extending their lives. Patients and doctors say that the drug’s power becomes evident almost immediately.Raphaelle Pereira, 22, had been waiting for years for a lung transplant in the Brazilian city of Curitiba. By 2021, her weight had dropped to 80 pounds, and she no longer had the strength to walk to the bathroom. Family members sold property and scraped together $54,000 to purchase a two-month supply of Trikafta in the U.S.“I took it for a couple of days, and then I just got up and said, ‘I think I’ll have a shower.’ My whole family was in shock,” she said. “A few days before I couldn’t even lift my arm.” With the data on how the medication had changed her condition, Ms. Pereira used a legal process to get Brazil’s public health system to buy a steady supply for her. She’s now working toward a career as a soccer commentator. Belinda Nell with photos of her sisters Lorryn and Jennifer, both of whom died of cystic fibrosis. Joao Silva/The New York TimesThe obstacles to getting Trikafta in the developing world go beyond the availability of the product. Huge numbers of patients remain undiagnosed. Those who do get diagnosed are unlikely to have access to expensive genetic testing to determine whether they have one of the mutations necessary for the drug to work.About 90 percent of patients of Northern European ancestry have the most common mutation needed for the drug to work, compared with far fewer people from the Middle East, Asia and Africa. In India, estimates range from 19 to 44 percent.Vertex is funding an academic project to better understand the genetics of cystic fibrosis patients in poorer countries. Dr. Milan Macek Jr., a geneticist in Prague, is working with doctors in lower-resourced countries to collect and analyze blood samples from willing patients. He has identified hundreds of diagnosed patients in Eastern Europe, the Middle East and Central Asia who have the most common mutation.Belinda Nell, who is working on the action in South Africa, followed the news about Vertex’s drugs closely, as her two sisters grew increasingly frail with cystic fibrosis.In 2014, Ms. Nell and her sister, Lorryn, who also had the disease, nursed a third sibling, Jennifer, as she was dying of it. Ms. Nell promised Lorryn that she would keep her from the same fate and, in early 2022, managed to obtain a couple months’ supply of Trikafta for her. But Lorryn’s lungs were too damaged, and she died last October.“It’s vital that children everywhere get access from a young age so they don’t endure the end stage like I saw with my sisters,” Ms. Nell said.Elif Ince
Read more →Her Foot Looked Normal. What Was Causing the Excruciating Pain?

A few weeks after she twisted her ankle, the girl’s foot kept getting worse. Her hand movements cued the doctor to a mysterious disease.The 9-year-old girl was strangely quiet throughout the meal. It was so uncharacteristic that in retrospect her father wasn’t sure why he didn’t notice. But he didn’t — until she started to scream. As tears ran down the girl’s face, she pointed to her foot, which was nestled in her lap.The man scooped his daughter into his arms and hurried out to his car. The crying stopped by the time they reached the urgent-care center near their hotel in Miami Beach, but her foot was still too painful to walk on.In the exam room, the father finally got a good look at his daughter’s foot. He was surprised: It looked completely normal. An E.R. doctor introduced herself and examined the limb. It looked OK to her too, and when the X-ray didn’t show anything, the doctor shrugged. If it keeps hurting, you should follow up with her doctor, she said.The father was baffled. The girl had twisted her ankle a few weeks earlier, but she was swimming and playing in the hotel pool most of the afternoon — enjoying the sun in this midwinter break before heading back to their home in New York City. But that night of pain was only the beginning. His youngest was a tough kid, but after the trip to Florida she complained about her ankle and foot just about every day. She had to sit out most of basketball season. She said it hurt too much to run.She had sprained that ankle several times over the past couple of years. Her doctors blamed weak ligaments and a sports-heavy schedule. They were an active family and recognized that injuries were just part of sports. But this was different. It seemed as if her ankle never got better after that last injury. Over the next few months, she saw a couple of orthopedists at the Hospital for Special Surgery. One ordered an M.R.I. of the ankle. That study was its own kind of nightmare. Holding her foot in the correct position was painful, the girl told them. And holding it still was practically impossible. Her foot had developed a tendency to roll to the side so that the arch and sole faced inward rather than down. And her toes were constantly in motion.The M.R.I. was unremarkable. Physical therapy helped the stiffness but didn’t straighten out her foot. A cortisone shot did nothing. Same with an ankle brace. How could all this grow out of a sprain, the parents asked each other. A rheumatologist was certain that this was juvenile rheumatoid arthritis. The blood tests said otherwise. As spring arrived, the young girl started using crutches to get around. Any weight-bearing was excruciating.Finally one evening, out of a sense of desperation, the father reached out to a high school friend, Joshua Hyman, who was now a pediatric orthopedic surgeon at NewYork-Presbyterian Morgan Stanley Children’s Hospital. He described his daughter’s pain and the strange stiffness that seemed to keep her foot on its side. There was a thoughtful silence on the phone, and then Hyman asked his friend if he was able to move his daughter’s foot — able to put it in a more normal position? He could, the father answered, but it felt as if the foot were fighting him. And as soon as the pressure was released, it would slowly turn back to its side. That’s how it felt best, his daughter told him.There was another pause. “Has anyone mentioned something called dystonia to you?” Hyman asked.A Wrong Message?Dystonia is a movement disorder characterized by persistent or intermittent muscle contractions, which cause abnormal, often repetitive movements or positions, Hyman explained. It can affect any part of the body, and in some cases the entire body. It’s a problem with the brain and the nerves. They send the wrong message to the muscles. There are lots of possible causes, Hyman added: medications, infections, brain injuries, a handful of inherited diseases. Dystonia? the father asked. He wasn’t sure he’d ever heard the word. How did she get this? Why did she get this? Is there a treatment? Hyman was sympathetic but couldn’t answer his friend’s many questions. For that they needed a neurologist — probably one specializing in movement disorders.It was late spring when the family got in to see Dr. Steven Frucht, director of the Fresco Institute for Parkinson’s and Movement Disorders at N.Y.U. Langone Health. As soon as he entered the exam room, Frucht noticed that the girl’s feet were asymmetric. She was sitting on a chair that was too tall for her feet to reach the floor, so they just hung down, at rest. The right foot was straight, as expected. The left pointed inward, toward the right, at a very unnatural angle. Frucht introduced himself and listened as the girl and her parents described her months of ankle pain.He asked if she could put her feet flat on the floor. It was easy to do with the right foot, but the left seemed to curve inward so that only the outer edge of the foot rested on the ground. And the big toe on the left foot moved up and down constantly. The toes on the right were still. “Why are your toes moving?” Frucht asked. “Because it’s uncomfortable,” the girl replied.Photo illustration by Ina JangRapping Her Knuckles on the TableFrucht asked if she had any problems with her hands. “Not really,” the girl answered. “Except I always get cramps when I write.” He gave her a pen and paper and asked her to write something for him. She had been writing for only a few seconds when she put down the pen and rapped her knuckles on the table. She then picked up the pen and started writing again. “Why did you do that?” Frucht asked. It feels better, she said.Frucht shared with the family the diagnosis he’d been considering since he first saw the child. There is a form of dystonia that, while rare, is the most common form of inherited limb dystonia seen in people of Ashkenazi Jewish descent. It is called DYT-TOR1A — named for the gene that is abnormal in this disease.“Whom could she have inherited it from?” the girl’s father asked. Neither parent nor anyone in either family had this problem. Frucht nodded; it is one of the mysteries of this disease. Only one parent has to have the gene to pass it on. Yet most people with this abnormal gene never develop the disease. No one understands why. Her father asked if it was her sports injuries that set her up for this. Probably not, the doctor replied, although there is still so much we don’t know. What we do know, he told them, is that this disease is often progressive. It had spread from her right hand to her left foot. And it may spread farther. Of course, they would need to do a test to see if she had this abnormality. Results would take about a week.When the test came back positive, the doctor started the girl on a drug called Artane, which blocks some of the brain’s abnormal signals to the body. As the dose was increased, the girl and her parents could see the difference. Her walk wasn’t completely normal, but it was much better — so much better that she was able to go to summer camp.But she had to keep increasing the dose of the medication. And by midfall she was starting to have side effects. Her performance in school, which had always been excellent, started to suffer. Frucht had told the family that there was another kind of treatment for this disorder, though he didn’t recommend it for younger children. It was something called deep brain stimulation. A small electrode could be implanted in the part of the brain where movement originates. Tiny electrical pulses would be generated at the site of the implant, and these pulses could block most of the abnormal signals that were driving the girl’s muscles to contract and jump. The parents were worried by the prospect of permanently implanting something in their daughter’s brain, but were even more worried by the progressive nature of this disease. The girl was excited by the prospect of not having to take a pill three times a day, but when one surgeon they saw said she would have to shave her head for the surgery, she immediately said no. She was quite proud of her long dark hair. Her parents kept looking. Finally they found a surgeon who had a lot of experience and would shave only a small patch of scalp.It took awhile, but the surgery has been life-changing. Or perhaps, the family would say, life-normalizing. Because she’s back: She’s back on the basketball court, back to her good grades. She still has her head of beautiful dark hair; and even the tiny patch that was shaved for the surgery is back.Lisa Sanders, M.D., is a contributing writer for the magazine. Her latest book is “Diagnosis: Solving the Most Baffling Medical Mysteries.” If you have a solved case to share, write her at Lisa.Sandersmdnyt@gmail.com.
Read more →Cancer patient's medical supplies donated to Ukraine

Published2 hours agoShareclose panelShare pageCopy linkAbout sharingImage source, Family handoutBy Emma Elgee and Steve Knibbs BBC NewsA cancer victim’s family has donated his unused medical supplies to Ukraine. Mark Lindesay, a pub landlord in Cirencester, was diagnosed with throat cancer and died in October. His sister Jenny Lockwood did not want the supplies to go to waste but was told the NHS could not use them due to rules about cross-contamination.Lukasz Woloszyn, a volunteer with Gloucester Ukrainian Aid has arranged instead to take the medical supplies to help people in war-torn Ukraine.Mark Lindesay, from Cheltenham, ran The Golden Cross pub since 2009 and was a “well-loved” member of the community.He was diagnosed with throat cancer in the summer of 2021 shortly after returning from a three-month stay in France. Mrs Lockward said: “He was very optimistic in everything he did. “He was always off to the next adventure and he was very interested in what was going on in the world.”He never complained, but the cancer was tough.”She said her brother had a tracheotomy and needed a feeding tube before his death, having lost the use of his voice. His cancer treatment meant he had thousands of pounds worth of medical supplies including syringes, dressings, medication and tubes. The UK Government has donated crutches, wheelchairs and other supplies to the frontline to help treat causalities of the Russian offensive and charities have also been donating supplies to the frontline. Mrs Lockwood said: “We saw the extent of it, all the tubes he needed, we don’t know what half of it is, most is sterile, in original packaging and can be used.”We tried talking to the district nurses and hospice but they didn’t know so we looked further afield for charities and actually found Lukasz.”The belongings were classed as medical supplies – not equipment- which meant they could not be taken back by the NHS due to infection control regulations. The NHS and charities in the UK do take back used equipment, such as crutches and wheelchairs, for reuse following an effort in 2018 to reduce the NHS’s carbon footprint. Mrs Lockwood said it was “fantastic” her brother’s supplies could be used anywhere but especially in Ukraine where there was a “real need”.”It is a way of helping out and maybe others will get the same idea and see this is something they can do,” she said.Lukasz Woloszyn works with Gloucester Ukrainian Aid – a volunteer force helping to support people in Ukraine. He said: “It will go straight to hospital, to frontline to help those people who will be injured.”That medical equipment will be very helpful as lots of people get injured and it’s very good stuff.”Things have changed – we are asked to take medical equipment, it’s quite important because it’s not only soldiers getting injured. “Private houses get bombed etc… so more stuff is needed.”We take out supplies at least once a month depending on the amount of stuff we manage to create for a journey.”He said the donations made a “big difference” to the people in Ukraine. Follow BBC West on Facebook, Twitter and Instagram. Send your story ideas to: bristol@bbc.co.uk More on this storyScottish medical supplies being sent to Ukraine2 March 2022Charity dispatches medical supplies for Ukraine21 November 2022UK donates vital medical supplies to Ukraine24 JanuaryHospitals send medical supplies to Ukraine4 March 2022Ukraine situation worse than thought – aid volunteer12 March 2022
Read more →The Medicine Is a Miracle, but Only if You Can Afford It
A wave of new treatments have cured devastating diseases. When the costs are too much, even for the insured, patients hunt for other ways to pay.April Crawford never thought she’d be begging for help on GoFundMe, but she has run out of options. She has multiple sclerosis, and Mavenclad, the drug that could slow her decline, has a list price of $194,000 a year. Her Medicare insurance will pay for most of it, but she has a co-pay of $10,000.Ms. Crawford, 47, doesn’t have $10,000 and has no way to get it. A law signed last year will put a $2,000 annual limit on out-of-pocket costs for Medicare patients like her — but not until 2025. Even at that price, money is tight in her household. She and her husband, who is disabled with COPD, live in Oliver Springs, Tenn., with a nephew who was disabled by a traumatic brain injury. All three of them rely on federal disability payments.So she posted an appeal on GoFundMe in August. At the time this article was published, she had raised $20.Ms. Crawford has come face to face with a persistent dilemma in medical care. Advances in science and immense investments by the federal government and drug companies have completely altered prospects for people with conditions that seemed untreatable in almost every area of medicine — cancers, allergies, skin diseases, genetic afflictions, neurological disorders, obesity.“This is the golden age of drug discovery,” said Dr. Daniel Skovronsky, chief scientific and medical officer of Eli Lilly and Company, which has new treatments for obesity, mantle cell lymphoma and Alzheimer’s.Prices reflect the inherently costly and fundamentally different way drugs are developed and tested today. But, he said, the burden on patients who cannot afford life changing new drugs weighs heavily on him and others who work for drug companies.For many people using private insurance, innovative medicines are dangling just out of reach. Even when Medicare’s 2025 cap comes into play — or the $9,100 cap that already existed for those receiving insurance under the Affordable Care Act — many will still find drugs unaffordable. Research suggests large numbers of patients abandon their prescriptions when faced with $2,000 in payments.One telltale sign that a treatment is working, experts say, is a widening chasm in outcomes between wealthy patients and everyone else. This is in part because when the prices for miracle drugs reach hundreds of thousands or even millions of dollars, many people do not fill prescriptions simply because they cannot afford them.Underlying the data that quantify these problems are individual stories about patients, like Ms. Crawford, who have tried desperately to find a way to pay for expensive drugs that could make a big difference in their lives. A few have succeeded, often briefly and tenuously, while many others do not. And those experiences produce consequences — cures only for a select few.Costly CuresThe new era in treating previously intractable diseases began with huge scientific leaps after the turn of the century, allowing researchers to find genes they could target to treat cancers and other diseases. Scientists could harness the immune system or suppress it and even alter patients’ very DNA with gene therapy.“Today’s drugs are more effective because they target the biology of disease ,” said Dr. Skovronsky of Eli Lilly, with few side effects.He called previous drugs to treat diseases like psoriasis or rheumatoid arthritis “blunt instruments” that shut down the immune system but had serious side effects.“Yesterday’s drugs were moderately effective in treating a broader population,” he added.But the drugs that have emerged often are extremely expensive to produce. At Lilly, Dr. Skovronsky said, the company will be spending more than $8 billion in 2023 on drug research and development.New Developments in Cancer ResearchCard 1 of 5Progress in the field.
Read more →