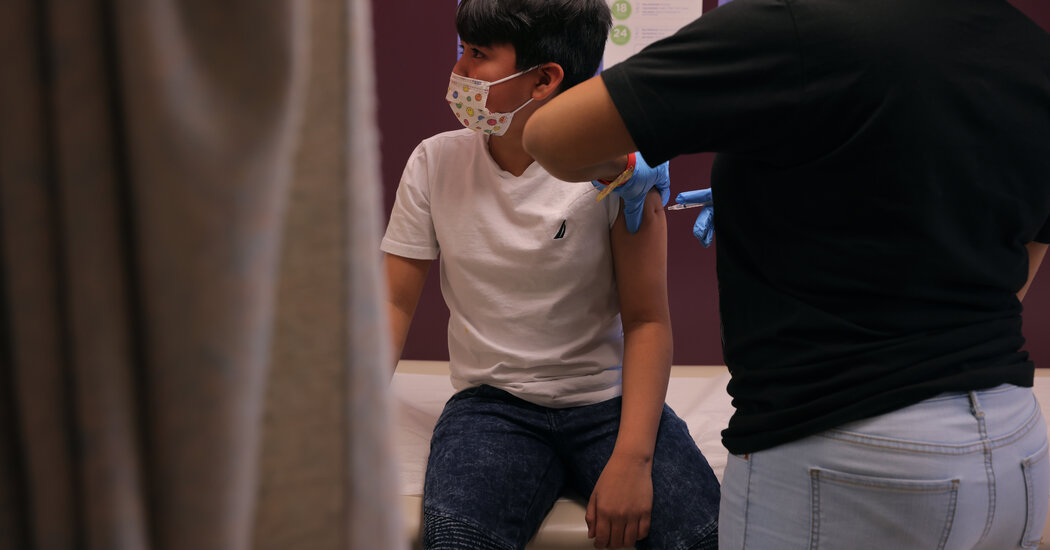
At one clinic serving low-income children, treatment for health problems that have gone unchecked during the pandemic is more in demand than coronavirus shots.CHARLOTTE, N.C. — Near the end of one of the first days that 5- to 11-year-olds could get a coronavirus shot last month, Dr. Anne Steptoe, a pediatrician, sat hunched in her cramped office between packages of diapers, onesies and children’s books, cataloging the week’s patients on her laptop.One teenage girl had been sleepless and suicidal; another was anemic. Several young boys had gained weight during the pandemic. A 10-year-old had been plagued by asthma attacks and was using her inhalers incorrectly. Another child of the same age needed a mental health consultation after angry outbursts at school.The rollout of the shot for young children brought relief for many families eager to shore up protection amid a wave of new virus cases. But much of the upfront demand has already been met; many parents who were eager to get their children vaccinated have done so. The success of the campaign, made even more urgent with the arrival of the Omicron variant, depends on the next phase: reaching the hesitant and undecided, including those who have not given thought or gained access to the shot.Dr. Anne Steptoe speaking to the staff at the Charlotte Community Health Clinic. A federal program called the National Health Service Corps brought Dr. Steptoe to the clinic last year as it was building out its pediatric unit, which had gone months without a pediatrician.Travis Dove for The New York TimesDr. Steptoe’s patients at Charlotte Community Health Clinic, many of whom have chronic medical conditions, crowded housing arrangements and vulnerable family members, are among the children most in need of the shot. Yet most parents who have brought their children to the clinic over the past month have declined it. They are wary of the vaccine, focused on getting treatment for mental and physical problems that had gone unchecked for much of the pandemic.More broadly, Dr. Steptoe said, her patients and their families were taking a cautious, “stepwise” approach, seeing how that shot was deployed among friends and neighbors, and asking for follow-up conversations with the clinic. That was also the case in the adolescent vaccination campaign, she said, leading to steadier uptake months into the shot’s deployment in that age group.For now, the numbers are meager. A pediatric vaccine kickoff event at the clinic drew just six children despite being advertised locally. Only 43 of the 900 doses the clinic received have been used as of Tuesday, and just 18 percent of 5- to 11-year-olds in Mecklenburg County, which includes Charlotte, had received an initial dose as of Nov. 29, said Dr. Raynard Washington, the county’s deputy public health director.While the Biden administration has paid special attention to getting the vaccine to pediatricians in private practice, it has also helped steer hundreds of thousands of doses to community health clinics like Dr. Steptoe’s. In 2020, 80 percent of Dr. Steptoe’s clinic’s nearly 5,000 patients were uninsured, including 70 percent of children. For them, it is one of the few local access points for health care in a fast-growing city.Already, Dr. Steptoe has seen the extremes of the pandemic’s effects on children’s well-being, including their mental health — the subject of a report published Tuesday by Dr. Vivek H. Murthy, the surgeon general.Josue, a 15-year-old from Honduras who had recently spent about six weeks in a hospital for malnutrition and blood count abnormalities, likely had undiagnosed cystic fibrosis, Dr. Steptoe decided after examining him.Dr. Steptoe speaking to Josue and his sister. Josue’s second dose of the Covid-19 vaccine, just a small piece of the care he needed, had been delayed.Travis Dove for The New York TimesShe reviewed with Josue and his sister a list of specialists he would need to see: a pulmonologist, geneticist, gastroenterologist, kidney doctor, endocrinologist and infectious disease expert. He was uninsured, and already facing what his sister said was a $2,800 hospital bill plus significant prescription drug costs, which Dr. Steptoe said a federal program could help cover.Josue had gotten his first coronavirus shot in early September, but was hospitalized before he was eligible for a second dose and had delayed it. For many patients seen at the clinic in the opening days of the children’s vaccine rollout — and their parents — the simple act of sitting in a physician’s office for the first time at least since the pandemic began forced a reckoning with vaccine hesitancy.“It’s building a plane in flight,” Carolyn Allison, the clinic’s chief executive, said of its efforts to get children vaccinated. “It may not be anti-vaccine, but ‘What is practical in my universe?’”Dr. Steptoe said she is careful to acknowledge a family’s fears about the Covid-19 vaccine without challenging them.Olivia Pelaez, a medical assistant at the clinic, prepared doses of Pfizer-BioNTech’s pediatric vaccine. Attempts to promote the vaccine have often been wedged into anguished discussions about how a child’s life had been disrupted by the virus.Travis Dove for The New York Times“What I’ve learned through the pandemic is just to keep having conversations and listening to people, because I do hear different things over time,” she said. Counseling families on the vaccine would be a “long-term game,” she said.Nationwide, five million of the 28 million children in the 5-to-11 age group, or roughly 18 percent, have received at least one dose of the Pfizer-BioNTech vaccine since it became available to them more than a month ago, a figure that suggests the campaign will require gradual progress.For the few young patients who did receive the Covid-19 vaccine at the clinic the first week they were eligible, families often made significant sacrifices to get them there. Emiliano, a 9-year old with attention deficit hyperactivity disorder who came for a physical, had recently lashed out several times at school. A clinic social worker discussed anger management with him. His father had taken a day off from work, and his mother three hours off, to get him there.But Emiliano eagerly agreed to the vaccine — prompting tears of relief from his mother, who had played him videos of other children getting it to encourage him.A patient’s view of the vaccine at any given appointment, Dr. Steptoe said, was a “snapshot in time.”Getting to a second conversation, or a third, increased her odds of a parent and child eventually choosing the vaccine.“Even for people that I know I have no shot of getting a shot into an arm that day,” she added. “It’s another voice, hopefully that they trust, or are building trust with, that says that in a calm and confident way and without any judgment.”Dr. Steptoe grew up in rural West Virginia without adequate primary care, she said, forcing her family to travel across state lines for routine checkups. She almost died after a botched tonsillectomy in elementary school — the surgeon did not properly close a wound — an experience that inspired her interest in pediatrics.“I knew from an early age that bad things happened to people in health care,” she said. “That was linked to the resources that we had in our community.”For many young patients, she said, the pandemic had sharpened conflicts within their families that had saddled them with mental health problems. As a screening question, she often asks patients whether they can count on the adults in their lives.The Coronavirus Pandemic: Key Things to KnowCard 1 of 4The Omicron variant.
Read more →