Researchers at Arizona State University have developed a breakthrough diagnostic tool that could transform how quickly and reliably we detect illnesses like COVID-19, Ebola, AIDS or Lyme disease. The test uses just a single drop of blood, costs a couple of dollars and delivers results in only 15 minutes.
In a new study, the researchers show the test can detect the virus that causes COVID-19 with pinpoint accuracy, clearly distinguishing it from other infections.
The new diagnostic device, called NasRED (Nanoparticle-Supported Rapid Electronic Detection), is simple and portable enough to be used almost anywhere — from remote rural clinics to busy urban hospitals. The tool provides lab-quality accuracy without expensive equipment and does not require specialized training, giving it the potential to become a public health game changer.
“We have the speed and ease of use of a rapid antigen test with sensitivity that’s even better than lab-based tests,” says Chao Wang, lead author of the new study. “This is very difficult to achieve.”
Wang is an associate professor with the Biodesign Center for Molecular Design and Biomimetics and ASU’s School of Electrical, Computer and Energy Engineering. He is joined by ASU researchers Yeji Choi, Seyedsina Mirjalili, Ashif Ikbal, Sean McClure, Maziyar Kalateh Mohammadi, Scott Clemens, Jose Solano, John Heggland, Tingting Zhang and Jiawei Zuo.
The research appears in the current issue of the journal ACS Nano.
Halting the spread of infectious diseases
Infectious diseases are one of humanity’s deadliest threats, causing immense suffering and economic damage worldwide. Collectively, infectious diseases cause over 10 million deaths around the world each year, and they are the leading cause of death in low-income countries.
Nearly 800,000 Americans die or are permanently disabled every year due to diagnostic errors, according to a study published in BMJ Quality & Safety. Many of these cases involve infections or vascular events that might have been treatable if caught early.
In many low- and middle-income countries, access to reliable diagnostic testing is limited or nonexistent. Expensive equipment, shortages of trained personnel and long turnaround times all contribute to delayed or missed diagnoses — often with deadly consequences.
A fast, affordable and portable test like NasRED would enable frontline health workers globally to detect infections early and respond before outbreaks spiral out of control.
“In many parts of the world, including the U.S., diseases are spreading, but people often don’t get tested — even for something like HIV. Ideally, you’d want to test them regularly, to catch infections early,” Wang says. “For example, people who use injection drugs are at higher risk for HIV or HCV, but they may be living in the streets and hard to reach. If we don’t test them consistently over time, we may miss the chance to intervene — until they develop serious complications like cancer or liver disease, when it’s much harder to treat.”
Striking diagnostic gold
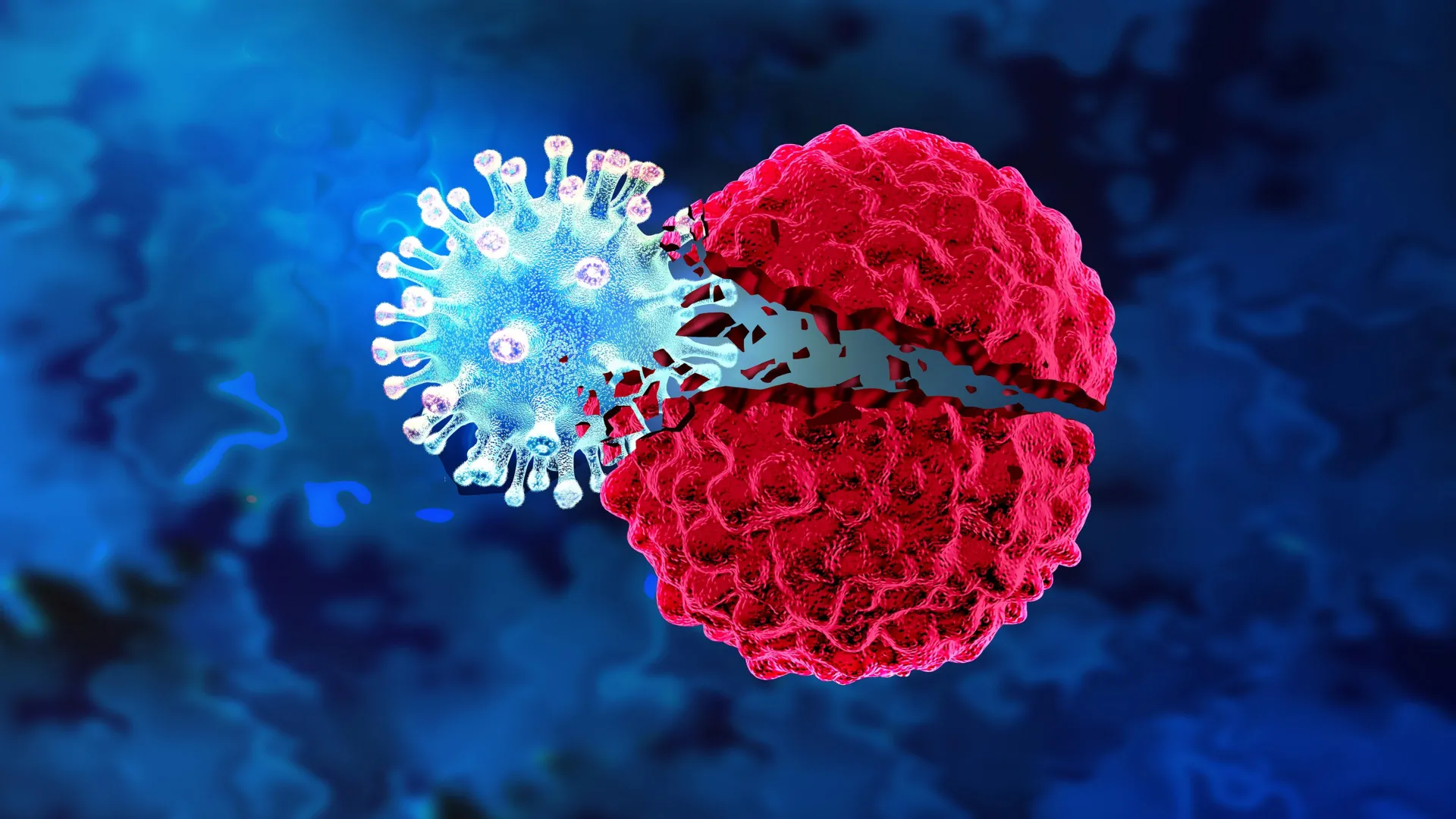
At the core of the new test are tiny gold nanoparticles, engineered to detect extremely small amounts of disease-related proteins. Researchers coat these nanoparticles with special molecules designed to detect specific diseases.
Some nanoparticles carry antibodies, tiny molecules that act like magnets. Antibodies stick to proteins released by viruses or bacteria when they infect the body. Other nanoparticles carry antigens, fragments of proteins taken directly from viruses or bacteria themselves. These naturally attract antibodies produced by the body to fight infections.
Once coated, these nanoparticles are combined with a tiny sample of bodily fluid, such as a drop of blood, saliva or nasal fluid. If a disease is present, most nanoparticles will sink to the bottom of the tube. If there is no disease, they will remain suspended throughout the liquid.
The NasRED device shines a small beam of LED light through the liquid at the top of the tube. The team built a custom electronic detector that senses how much light gets through the tube. More light means the nanoparticles have sunk to the bottom, leaving the top fluid clearer, meaning that the disease is present.
Accurate, accessible and affordable
The device is so sensitive it can detect disease even when only a few hundred molecules are present in a tiny fluid sample — just a fraction of a single drop. This is a concentration nearly 100,000 times lower than what standard laboratory tests require.
Adding to its promise is NasRED’s portability and affordability. The current gold standards for testing, like PCR or ELISA, require expensive equipment and trained technicians. NasRED is compact and user-friendly. The researchers estimate each test costs $2, making it ideal for use in low-resource or remote locations.
NasRED has the potential to fill a critical diagnostic gap, especially for diseases that are difficult to detect early, such as hepatitis C, HIV or Lyme disease. It is also promising for emerging outbreaks with low prevalence but high risk. Such diseases often go undiagnosed because running a lab test for just one or two patients isn’t cost effective. NasRED bridges that gap by offering a highly sensitive test that works immediately and economically at the point of care.
While NasRED currently requires small, benchtop machines for spinning and mixing samples, the researchers are working to further miniaturize and automate the process. With continued development, the technology might one day become a convenient home test, similar to existing rapid COVID-19 tests. However, it would have vastly superior sensitivity and broader applications.
Significant leap forward in diagnostics
NasRED dramatically surpasses existing diagnostic standards. The new study shows that NasRED is roughly 3,000 times more sensitive than ELISA, requires 16 times less sample volume, and delivers results approximately 30 times faster.
An earlier version of the technology detected Ebola in a tiny sample of blood. “For the new technology, we pushed the sensitivity down to the attomolar range,” Wang says. That’s like detecting a single drop of ink in 20 Olympic swimming pools.
The technology holds promise for detecting viral loads directly from bodily fluids without the complicated sample preparation used in PCR-based methods. In preliminary tests with actual coronavirus particles, NasRED achieved sensitivities comparable to Abbott ID NOW, a popular molecular test for many diseases such as COVID-19.
“One of the strengths of our sensor is that it’s highly modular,” Wang says. “The nanoparticles are designed so that we can easily swap in different proteins, allowing the same platform to be adapted for many different diseases. We’ve already demonstrated this approach in our research on Shiga toxin-producing E. coli, as well as cancer biomarkers, Alzheimer’s-related proteins, Lyme disease and African swine fever.”
Wang recently received the Bay Area Lyme Foundation Emerging Leader Award and will make use of the high sensitivity and portability of this new technology to detect early Lyme infection.
As the technology evolves, its range of applications may extend beyond infectious diseases. Early detection of cancers, real-time monitoring of chronic illnesses and improved surveillance of public health threats are all within reach.
Read more →