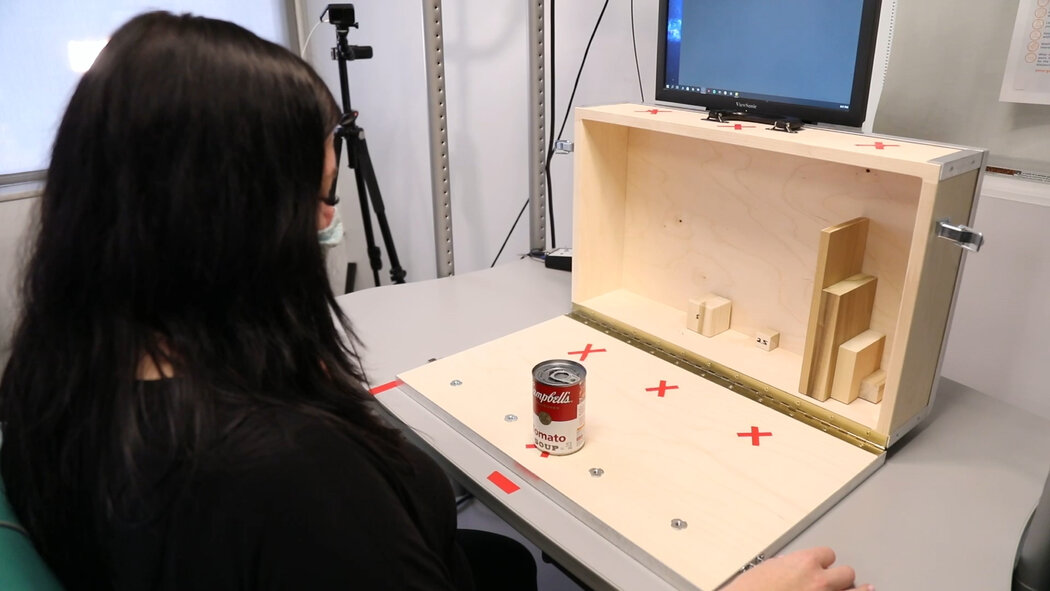
When the idea struck him, nearly 50 years ago, Dr. Étienne-Émile Baulieu believed it could be revolutionary. Creating a pill that could abort a pregnancy would transform reproductive health care, he thought, allowing women to avoid surgery, act earlier and carry out their decisions in private.“When science meets women’s cause, it is irresistible,” Dr. Baulieu, 96, a French endocrinologist and biochemist often called the father of the abortion pill, said on a recent Sunday afternoon in his apartment in a century-old building a short walk from the Eiffel Tower.He had also hoped, as he wrote in a 1990 book, that by the 21st century, “paradoxically, the ‘abortion pill’ might even help eliminate abortion as an issue.”That prospect seems as distant as ever, especially in the United States. Not only has abortion remained fiercely contentious since the pill Dr. Baulieu spearheaded, mifepristone, was approved in America in 2000, but last year’s Supreme Court decision ending the federal right to abortion has divided the country over the issue as never before.Yet over time, some of Dr. Baulieu’s other expectations have materialized. Today, medication abortion, in which mifepristone and a second drug are taken early in pregnancy, is used in over half of pregnancy terminations in the United States. That proportion is expected to increase, even in states that have banned abortion, where growing use has put the pills at the center of legal and political battles.For Dr. Baulieu, who continues work in his lab on the southern rim of Paris, his office overlooking a former asylum where the Marquis de Sade was held, the volatile developments are just the latest turns in an eventful life. He transported guns as a teenager in the French Resistance during World War II, changing his name and taking refuge high in the Alps. He joined the Communist Party and then quit it in 1956 after the Soviet invasion of Hungary. And he socialized with the artists Andy Warhol and Jasper Johns in the 1960s, beginning a pattern of friendships with painters, sculptors, musicians and actors that he said had helped inspire his scientific work.Dr. Baulieu continues to work at his lab at the Kremlin-Bicêtre Hospital on the southern edge of Paris. Julie Glassberg for The New York TimesMifepristone, typically followed by misoprostol, is now used in more than half of U.S. pregnancy terminations.Gabriela Bhaskar for The New York TimesThat work has earned Dr. Baulieu many scientific honors, including the Lasker Award, often considered the most prestigious American prize in medicine. Recently, France’s president, Emmanuel Macron, awarded him the Grand Cross of the Legion of Honor, the highest distinction. Admirers have floated his name for a Nobel Prize.For his leading role in developing mifepristone, he has been hailed as a visionary by abortion rights supporters and vilified as an incarnation of Hitler by abortion opponents, a charge that he said he found especially jarring because he is Jewish.Although he and the pill have become lightning rods, Dr. Baulieu speaks of the abortion debate without vitriol, cognizant of the complexity of the issue.“When he believes something, he’s quite relaxed,” said Simone Harari Baulieu, who has been his romantic partner for over 25 years and became his second wife in 2016.With a medical degree and a Ph.D. in biochemistry, Dr. Baulieu has always considered himself “a doctor who practices science,” looking for ways to translate research into useful applications.Scientifically and medically, “women are not enough understood,” he said, adding: “I like women. Why not?”An independent streakDr. Baulieu’s office is jumbled with memorabilia, papers, books, art and a chalkboard with sketches of how the brain processes memories.Julie Glassberg for The New York TimesEclectic artifacts fill the home Dr. Baulieu shares with his wife, who runs a film and television production company.In a portrait by the photographer Richard Avedon, Dr. Baulieu wears a black turtleneck and holds a small white pill. A surrealist painting of him and Ms. Harari Baulieu by the contemporary French artist Gérard Garouste hangs above an ornate fireplace.Shelves overflow with books: Maimonides’s “The Guide for the Perplexed”; a history of “Old Shanghai”; a collection of excerpts from Proust. More books are piled on the living room’s parquet wood floor, near windows overlooking a narrow balcony edged by an ornamental iron railing.On the dining room table are two recent gifts from Vice President Kamala Harris. Her late mother, Shyamala Gopalan Harris, a breast cancer researcher, spent about a year working in Dr. Baulieu’s lab in the 1980s, collaborating with him on research about estrogen and a mammary gland protein. (She did not work on the abortion drug.)On an official trip to France in 2021, the vice president met privately with Dr. Baulieu and his wife. She gave them a glass bowl and the French translation of her book, inscribed: “Thank you for your friendship and all you do and mean to our family. Love, Kamala.” Last month, in remarks at a luncheon for Mr. Macron in Washington, Ms. Harris mentioned her mother’s work with “the legendary French Professor Baulieu.”Dr. Baulieu’s instinct for innovation may have come from his father, Dr. Léon Blum, a kidney specialist who was one of the first doctors to use insulin for diabetics and who treated an Egyptian king’s diabetes while on his honeymoon with Dr. Baulieu’s mother.In World War I, Dr. Blum, who was from German-occupied Alsace, was drafted by the German Army. But he surreptitiously aided France by asking German officers he treated to mail him postcards about how much urine they were producing; he used the postmarks to gauge German troop movements and gave that intelligence to the French military. Eventually, he fled to France, where he was awarded the Legion of Honor.He died at age 54 when his son, born Étienne Blum, was only 3. Étienne’s mother, Thérèse Lion, a lawyer and conservatory-trained pianist, moved her three children to Paris.“She believed that my father died because of contamination from sick people,” Dr. Baulieu said. She told him he could become anything he wanted, except a doctor. “And the only thing I chose was to become a physician,” he said.Photos in Dr. Baulieu’s office show him with his father, left, Léon Blum, a kidney specialist, and his mother, Thérèse Lion, a lawyer and pianist.Julie Glassberg for The New York TimesMax-Fernand Jayle, who studied hormonal processes in women, was a mentor to Dr. Baulieu and gave him opportunities early in his career.Julie Glassberg for The New York TimesHis independent streak was honed long before that, though. During World War II, his family fled German-occupied Paris for Grenoble, and at 15, he and classmates distributed anti-Nazi leaflets and “threw stones at people who were working for Germans,” he said.Two years later, he was in a cafe when he noticed men lurking outside and realized, “I was detected by the Germans.” He slipped out the back and left town without saying goodbye to his mother.When he joined French Resistance members in the alpine towns of Chamonix and Annecy, they suggested he change his name, offering several options, including “Beaulieu,” which means “beautiful place.” He liked that, but felt it would be pretentious to adopt “beautiful” as a name, so he changed the spelling to “Baulieu” and chose “Émile” as a first name.His group’s activities included ferrying arms and kidnapping and executing an imprisoned Vichy official.“I was too young to shoot,” Dr. Baulieu said, “so they gave me a camera,” which he used to photograph the execution.“I hated the violence, but they were really enemies and traitors,” he said.Like fellow French Resistance members, he joined the Communist Party but declined to become a party official after the war. Instead, he went to medical school.He joined the lab of a scientist, Max-Fernand Jayle, who had been blinded during an experiment. Dr. Baulieu said other students thought working for Dr. Jayle would be a career dead end, but he considered Dr. Jayle inspiring and original.An encouraging mentor, Dr. Jayle, who studied hormonal processes in women, gave Dr. Baulieu advanced opportunities that allowed him to become a tenured professor at 31.In an important early discovery that had eluded many scientists, Dr. Baulieu determined how to detect a hormone, dehydroepiandrosterone, or DHEA, which helps produce estrogen and testosterone and can signal diseases like adrenal cancer.“I did it with a simple idea which, in classical terms, made little sense,” he wrote. Instead of looking in oily extracts from the adrenal glands, he found a water-soluble form in urine, “like probing a vinaigrette: looking in the vinegar instead of the oil.”Vice President Kamala Harris gave Dr. Baulieu a bowl emblazoned with the vice presidential seal. Her mother, Shyamala Gopalan Harris, a breast cancer researcher, spent about a year working in Dr. Baulieu’s lab in the 1980s.Pam Belluck/The New York TimesA sculpture, called “Nana,” with parts by Niki de Saint Phalle, left, and Jean Tinguely, right, in Dr. Baulieu’s office.Julie Glassberg for The New York TimesThat earned him an invitation to spend a year at Columbia University with Dr. Seymour Lieberman, a steroid expert. But Dr. Baulieu’s previous Communist ties led the Eisenhower administration to repeatedly reject his visa application, despite pleas from fellow scientists, and he obtained a visa only after John F. Kennedy became president.On the ship to New York in 1961, Dr. Baulieu met Barbara Rose, a prominent art historian. She introduced him to up-and-coming artists, including Frank Stella (whom she later married), Mr. Johns, Mr. Warhol and Robert Rauschenberg.“I realized from my artist friends the similarity of creation in science and art,” Dr. Baulieu wrote.His admiration for creative people endured, leading to close friendships and occasional romances. During his long marriage to his first wife, with whom he had three children, he had several romantic relationships, he said, adding, “I knew a number of beautiful, interesting, intelligent and free women.”One relationship was with Niki de Saint Phalle, whose riotously colorful paintings and sculpture are displayed in his home and laboratory office. In the late 1970s, at the French Riviera home of the conductor Herbert von Karajan, Dr. Baulieu met the actress Sophia Loren, and he said they had a romantic relationship while both were married to other people. At one point, they were photographed in a car. “I was in love, yes,” Dr. Baulieu said. The relationship ended, he said, because she was devoted to raising her children and wanted to preserve her marriage. A representative for Ms. Loren declined to respond to questions. In 1991, Ms. Loren told Vanity Fair, “I was never involved with him.”An ‘unpregnancy pill’Dr. Baulieu in 1984, holding an abortion pill.Arnaud Borrel/Gamma-Rapho, via Getty ImagesDr. Baulieu’s path to developing the abortion pill began in 1961 with a speaking invitation from Gregory Pincus, who helped invent the birth control pill. Dr. Pincus, then a co-director of the Worcester Foundation for Experimental Biology in Massachusetts, became another mentor. He suggested that Dr. Baulieu travel to Puerto Rico to observe clinical trials of the contraceptive pill.“When I saw what they were doing in Puerto Rico, it was remarkable for the treatment of women,” Dr. Baulieu said.Back in Paris, Dr. Baulieu, who directed a unit at France’s National Institute of Health and Medical Research, rejected an offer to become head of research at the pharmaceutical company Roussel-Uclaf, but agreed to become a part-time consultant. The arrangement allowed him to use some company laboratories and molecules for research but barred him from earning money from any Roussel-Uclaf products.He began thinking of potential advances in reproductive medicine. During his medical residency, he’d learned that some women seeking to terminate pregnancies would insert sticks to cause miscarriages and would then go to the hospital. He was shocked that some surgeons instructed employees not to give anesthesia. “‘Teach her a lesson she’ll remember,’ I heard one of them say,” he wrote.In 1970, Dr. Baulieu was visiting India with a group of intellectuals when a woman begging on a bridge in Kolkata, then known as Calcutta, approached him while cradling her dead baby and holding the hand of a child who held another one of her children.“It really caused an emotion for me, which has persisted all my life,” he said. “I think always of Calcutta as something which has pushed me to really work hard.”He started brainstorming an idea for an “unpregnancy pill.” It would involve a kind of biological sleight-of-hand.The lab at Kremlin-Bicêtre Hospital.Julie Glassberg for The New York TimesDr. Baulieu described the work of RU-486 as “contragestion” because it counteracted the gestation process. More simply, he wrote, “RU-486’s action is like jamming a radio signal.”Julie Glassberg for The New York TimesThe hormone progesterone is pivotal in pregnancy because it prepares the uterus to receive and hold an embryo. What if progesterone could be prevented from delivering its cellular messages?“I wanted to create an anti-hormone,” Dr. Baulieu said.In guinea pigs, his team identified receptor molecules that progesterone connected with to convey messages. Dr. Baulieu suggested trying to make a faux progesterone, an impostor to latch onto progesterone receptors so the real hormone could not.He asked Roussel-Uclaf’s chemists to try grafting a cluster of atoms onto a molecule with progesterone’s structure so it would be similar enough to bind to the progesterone receptor.The leader of the German company that was Roussel-Uclaf’s majority stakeholder, Hoechst AG, was a staunchly anti-abortion Catholic, Wolfgang Hilger. To avoid controversy in meetings with company officials, Dr. Baulieu said, he emphasized a non-abortion-related property of an antiprogesterone compound: Because it would also block receptors for the stress hormone cortisol, it could theoretically treat burns, wounds, glaucoma and other conditions.In 1980, Roussel-Uclaf’s chief chemist, Georges Teutsch, synthesized a compound that worked as Dr. Baulieu had envisioned.“Although neither Teutsch nor most of the others in the company initially realized it, it was also what I wanted: an antiprogesterone,” Dr. Baulieu wrote. Registered as Roussel-Uclaf 38486, the company’s 38,486th molecule, it was nicknamed RU-486.“It’s like a key in a lock,” Yvette Akwa, a researcher in Dr. Baulieu’s lab, explained recently. “You make a similar key that fits the lock. And then when progesterone would go to open the door, it can’t because it’s already blocked.”Dr. Baulieu called the concept “contragestion” because it counteracted the gestation process. More simply, he wrote, “RU-486’s action is like jamming a radio signal.”After other scientists tested RU-486 on rats and monkeys, Dr. Baulieu urged Roussel-Uclaf to allow human trials and asked an obstetrician-gynecologist friend in Switzerland, Dr. Walter Herrmann, to conduct them. In 1982, a trial found that RU-486 aborted early pregnancies in nine of 11 patients. Later trials showed that by following RU-486 with a prostaglandin, a medication that causes contractions, the method was about 95 percent effective. Today, RU-486 — mifepristone — is followed 24 to 48 hours later by a synthetic prostaglandin called misoprostol.A demonstration against RU-486 outside the headquarters of Roussel-Uclaf in Paris in 1991.Jean-Michel Turpin/Gamma-Rapho, via Getty Images“Up to then, abortion had not been proposed in a way which, at the same time, is efficient, safe and not too difficult for women,” Dr. Baulieu said.Abortion opponents pilloried the company, swarming a shareholders’ meeting. Drawing analogies to Hoechst’s predecessor company, I.G. Farben, which made the cyanide gas used in Nazi death camps, some shouted, “You are turning the uterus into a crematory oven,” Dr. Baulieu wrote.In Washington, an anti-abortion campaign flooded the French Embassy with letters threatening to boycott French products if France approved the pill. The company almost withdrew its application. In September 1988, the French authorities approved RU-486.Several days later, debating Dr. Baulieu on French television, Dr. Jérôme Lejeune, an anti-abortion pediatrician who discovered the genetic basis of Down syndrome, called RU-486 “the first anti-human pesticide” and said it would “kill more human beings than Hitler, Mao Zedong and Stalin combined.”“You can’t say it’s like Hitler,” Dr. Baulieu exclaimed. “Don’t say things that would make me laugh if this weren’t a serious debate.”The clamor from opponents was so intense that a month after the approval, Roussel-Uclaf said it would stop marketing RU-486. Dr. Baulieu wrote that the company’s chairman, Dr. Edouard Sakiz, told him that he feared a violent incident, like one that month when an ultraconservative group set fire to a Paris movie theater showing “The Last Temptation of Christ.”But Dr. Sakiz told Dr. Baulieu he was free to speak out. Dr. Baulieu flew to Brazil for the World Congress of Gynecology and Obstetrics, where doctors and researchers vehemently decried Roussel-Uclaf’s withdrawal of RU-486.Soon afterward, Claude Évin, the health minister of France, which owned part of Roussel-Uclaf, called RU-486 “the moral property of women” and pressured the company to resume selling it. “I could not permit the abortion debate to deprive women of a product that represents medical progress,” he said.A poster advertised a conference Dr. Baulieu spoke at in China in the 1990s.Julie Glassberg for The New York TimesDr. Baulieu in his uniform from the French Academy of Sciences.via Étienne-Émile BaulieuAfter RU-486’s approval, Dr. Elisabeth Aubény, an obstetrician-gynecologist, said her hospital gave it to appreciative patients, but also encountered protesters who chained themselves to operating tables.Beginning in the 1980s, Dr. Baulieu received hate mail, some of it antisemitic. A poster in Canada featured Dr. Baulieu’s photo and the words “Wanted for Genocide.” One in San Francisco equated him with the Nazi death camp doctor Josef Mengele, calling them “blood brothers.” In New Orleans, a small bomb exploded at a conference at the time Dr. Baulieu would have been speaking if not for travel delays, he said.He also received grateful letters from America and pleas for the pill to be available there. Some at Roussel-Uclaf felt he hadn’t shared enough credit for RU-486. Not long after Dr. Baulieu won the Lasker Award, Dr. Teutsch, the chemist, was quoted as saying, “Étienne Baulieu is the father of the pill, but he is not the father of the compound.”For years, afraid that opposition in America would lead to boycotts of its other products, the company declined to seek approval of RU-486. In 1993, an abortion rights organization started a clandestine lab to make the pill in a suburban New York warehouse. In 1994, with the Clinton administration championing the pill, Roussel-Uclaf donated American rights to the Population Council, a nonprofit organization.The Food and Drug Administration gave RU-486 conditional approval in 1996, but large pharmaceutical companies wouldn’t manufacturer it, and full approval didn’t occur until 2000, after a small company, Danco Laboratories, agreed to make it.Today, as some states ban nearly all abortions and propose actions to target medication abortion, other states and the Biden administration have taken steps to expand access to abortion pills. Patients can have consultations with abortion providers via telemedicine and receive the prescribed pills by mail. A new F.D.A. rule will allow retail pharmacies like CVS to fill prescriptions for the pills. And in states with abortion bans, many patients order pills from an overseas telemedicine abortion organization.Still at workThe building containing Dr. Baulieu’s lab is named for one of his mentors: Gregory Pincus, an American scientist who helped invent the birth control pill.Julie Glassberg for The New York TimesThese days, scientific experimentation continues apace at Dr. Baulieu’s lab in the Grégory Pincus building, a boxy, teal-colored structure on a hospital campus that was previously the site of an 18th century prison.Dr. Baulieu has made discoveries about various steroid hormones, including the finding that some are synthesized in the brain; he called them “neurosteroids.” Today, his team studies Alzheimer’s and has started clinical trials on a new method to treat severe depression, based on Dr. Baulieu’s ideas about a receptor for a particular neurosteroid.“He discovered both the receptor and the function,” said Isabelle Villey, a biochemist who leads a small company headquartered at Dr. Baulieu’s lab.Dr. Baulieu’s office is jumbled with memorabilia, papers, books and art. Near a chalkboard with sketches of how the brain processes memories, there are avant-garde sculptures by his artist friends — including a mechanized representation of the sword he received upon being inducted into the French Academy of Sciences, where he later served as president. Recently, warmed by a scarf and a puffy down vest under a blazer, he gave an impromptu seminar, thumbing through one of his RU-486 articles.He remains energetic, barely slowed by his use of a cane and displaying only occasional hiccups in memory.Over dinner at a Montparnasse seafood restaurant, Dr. Baulieu said he was dismayed by anti-abortion politics and what he called the “scandalous” Supreme Court ruling in America. But, he said, “it’s good that my pill is accepted by a large number of women.”His outlook has been shaped by living nearly a century, marked by war, social upheaval and scientific innovation.“I’m optimistic,” Dr. Baulieu said, “because science helps you to be optimistic.”In his office, Dr. Baulieu gave an impromptu seminar about one of his scientific papers on RU-486.Julie Glassberg for The New York Times
Read more →