
Helping Stroke Patients Regain Movement in Their Hands
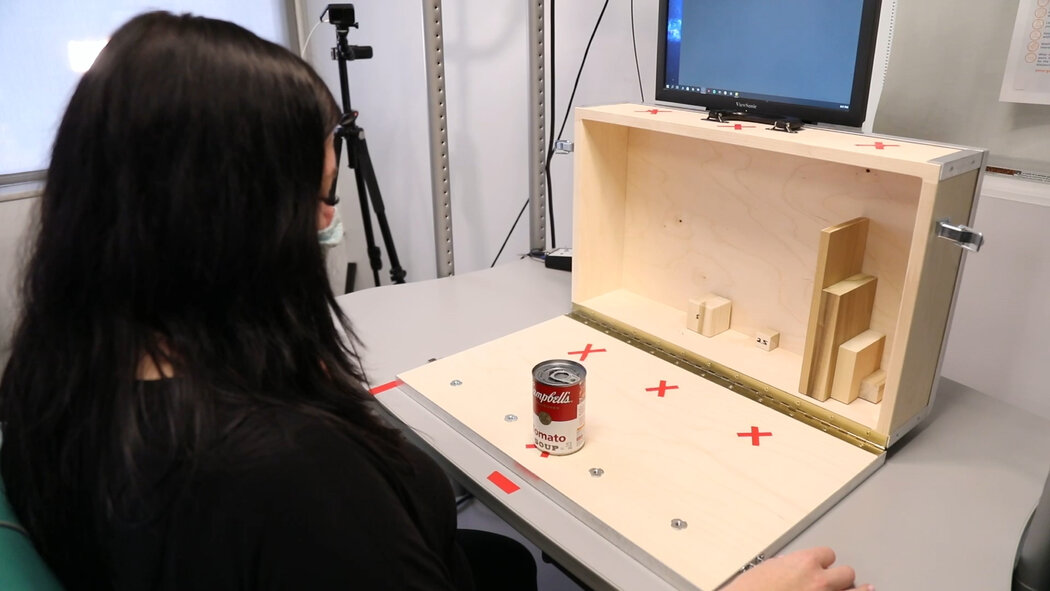
Heather Rendulic was 23 when she suffered a stroke that disabled her left side. Ten years later, her left arm and hand remain so impaired that she cannot tie her shoes, type with two hands or cut her own food.But for an extraordinary month, while participating in an innovative study, she suddenly was able to open a padlock with a key, draw a map of Italy, dip a chicken nugget in sauce and eat it with a fork — all with that left hand.“It was like I actually had two arms, oh my gosh!” Ms. Rendulic said recently.Researchers from the University of Pittsburgh and Carnegie Mellon University implanted electrodes along her spinal cord , delivering electrical stimulation while she tried different activities. With stimulation, her left arm had greater mobility, her fingers had more dexterity, and she could make intentional movements more quickly and fluidly.The study, published Monday in the journal Nature Medicine, represents the first successful demonstration of spinal cord stimulation to address weakness and paralysis in the arms and hands of stroke patients.The study was small and preliminary, involving only Ms. Rendulic and another patient. Several scientists said many questions remain about the technique’s effectiveness and applicability, but that the research suggested spinal cord stimulation could eventually help some of the many people who experience strokes.“I think there’s enormous implications for improving quality of life,” said Dr. Lumy Sawaki-Adams, the program director in the clinical research division of the National Institute of Neurological Disorders and Stroke, who was not involved in the research. Still, she said, “we have to be cautious that we’re not offering hope to many people when I think we’re not there yet.”Spinal cord stimulation has been used for decades to treat chronic pain. More recently, experiments delivering stimulation — either through surgically implanted electrodes or noninvasively through electrodes placed on the skin — have shown promise in helping patients with spinal cord injuries regain mobility in their legs and, in some cases, their arms and hands.But the approach has been mostly unexplored for stroke, partly because of differences in the location and type of damage, neurological experts said.Because strokes occur in the brain, it had been assumed that applying stimulation outside the brain would not provide “the same bang for the buck,” said Arun Jayaraman, the executive director of the technology and innovation hub at Shirley Ryan AbilityLab, a rehabilitation center in Chicago. He said the study, which he was not involved in, countered that assumption, instead suggesting that stimulating the spine, the pathway from the brain to hand and arm muscles, may help impaired limbs.Over four weeks, Ms. Rendulic was given increasingly challenging tasks to perform, like grasping and moving a soup can. “I immediately was opening and closing my hand,” she said. “We all broke down in tears.”Powell et al., University of Pittsburgh and Carnegie Mellon UniversityEach year, more than 12 million people worldwide and nearly 800,000 in the United States experience strokes, said Dr. Karen Furie, the vice chair of the American Stroke Association’s stroke brain health science subcommittee.Initially, patients typically receive about six months of physical, occupational and other therapies, she said, but then progress often plateaus.“We have virtually nothing to offer people who are years out and have longstanding disabilities,” said Dr. Furie, who is also the chair of neurology at Brown University’s Warren Alpert Medical School and was not involved in the study.About three-quarters of stroke patients experience impairment, weakness or paralysis in their arms and hands, said Dr. Elliot Roth, an attending physician at Shirley Ryan AbilityLab’s Brain Innovation Center, who was not involved in the study. “For many people, it’s the toughest part of the stroke recovery process and tends to recover the slowest,” he said.The patients who participated in the study had experienced different types of strokes and had varying degrees of impairment. Ms. Rendulic’s stroke was hemorrhagic, caused by bursting blood vessels. The other, more severely impaired patient, a 47-year-old woman whom researchers did not identify, experienced an ischemic stroke, which is more common and involves blocked blood vessels.Researchers implanted strands of eight electrodes in two locations, corresponding to where neurosensory fibers from the arm and the hand enter the spinal cord.Marco Capogrosso, an assistant professor of neurological surgery at the University of Pittsburgh, said that the approach derived from the fact that with strokes, some neural areas remain undamaged.“So, if we can build this technology to amplify neural signals, maybe we have a chance to restore arm and hand movement,” said Dr. Capogrosso, who led the research with Elvira Pirondini, an assistant professor of physical medicine and rehabilitation at the University of Pittsburgh, and Douglas Weber, a professor of mechanical engineering at Carnegie Mellon’s Neuroscience Institute.Five days a week for four hours each day, researchers activated the stimulation, calibrated it to determine optimal parameters for each patient and asked them to attempt various movements and tasks. Right away, the effect was noticeable.“The very first day in the lab and the first time they turned it on, I was sitting in a chair, and they asked me to open and close my hand, and that’s something that’s really difficult for me,” Ms. Rendulic said. As her husband and mother watched, “I immediately was opening and closing my hand,” she said. “We all broke down in tears.”Ms. Rendulic said she would welcome another opportunity to have spinal cord stimulation. “I did threaten to not show up to the surgery to get it removed,” she said. “I just wanted it all the time.”Kristian Thacker for The New York TimesOver four weeks, she was given increasingly challenging tasks, like gripping and moving a soup can. With stimulation, her left hand moved 14 small blocks over a barrier in a box, compared with six blocks without stimulation.Typically, when Ms. Rendulic, 33, who works at home for a company’s human resources department, tries to make her left hand do something like grasp a pen, her arm feels like “it’s made of rock,” almost disconnected from her brain, she said. With stimulation “it was like my brain was able to find my left arm so much easier.”The other patient, who was given simpler tasks because her left hand was almost completely paralyzed, improved in skills like reaching.Researchers also tested a “sham” stimulation, activating electrodes randomly to see if patients responded to a kind of placebo effect rather than stimulation targeted specifically to their arms and hands. Both performed better with targeted stimulation.The patients sensed the stimulation, but it didn’t cause pain, rigidity or safety problems, researchers reported.The approved study protocol required removing the electrodes after 29 days. But one month later, the patients retained some improved abilities, surprising researchers. “We thought it was not possible” after only four weeks of stimulation, Dr. Pirondini said.It is unclear exactly why the benefit can persist, Dr. Capogrosso said, but he hypothesized that “the same neural processes that allow these people to use this stimulation method also lead to a recovery of movement when the stimulation is off.” He added, “we’re not creating new fibers, but we’re definitely restrengthening what there is.”Several experts noted that this pilot study was not designed to answer the most relevant question for patients: Can the improvements in laboratory tasks translate into skills that matter in daily life?“It’s a first step among hundreds,” said Dr. Daniel Lu, a professor and vice chairman of neurosurgery at the University of California Los Angeles, who co-authored a 2016 study that showed that spinal stimulation from implanted electrodes improved hand strength and control in two spinal cord injury patients.Dr. Lu said he believes stimulation is promising, but that its impact in the new study was difficult to evaluate because there was no comparison group and patients were not given the same regimen of intensive activities before stimulation — activities that might themselves have therapeutic benefit.“Is it possible that you’re just exercising the patient, and the patient without the stimulation would have gotten the same effect?” he asked.While Ms. Rendulic has devised ways to do activities like driving and typing with only her right hand, everyday frustrations rankle. But, “In the trial, I did get to cut up a steak, which was awesome,” she said.Powell et al., University of Pittsburgh and Carnegie Mellon UniversityAnother question neuroscientists raise is whether — or in what circumstances — it is better to surgically implant electrodes or place them on the skin, a less expensive method called transcutaneous stimulation. The new study’s authors consider surgical implantation superior because it is “much more specific,” said Dr. Weber, allowing it to “target the muscles that control the wrist and the hand.”Others, like Chet Moritz, a professor of neurotechnology at the University of Washington, have reported improvements in spinal cord injury patients using electrodes on the skin, including benefits lasting months after stimulation ends. “It’s true we can’t tune the shoulder to this degree and the elbow to this degree and the wrist to that degree, but the nervous system seems to take care of that for us,” he said.Several neurological experts predicted that both methods could eventually be helpful and appropriate for different patients, depending on their health and other factors. All the experts, including the study authors, said stimulation would be more effective if accompanied by rehabilitation therapies.The study’s authors said their continuing research is evaluating patients of varying stroke severity, age and other characteristics to determine who would benefit from their approach. They have formed a company and said they envision that, as with similar technology for chronic pain, patients could adjust their stimulation via app or remote control.If stimulation becomes regularly available to stroke patients, Ms. Rendulic would welcome it. “I did threaten to not show up to the surgery to get it removed,” she said. “I just wanted it all the time.”While she has devised one-handed ways to do activities like driving and typing, everyday frustrations rankle, like needing her husband Mark, whom she calls “my left-hand man,” to slice steak for her.“In the trial, I did get to cut up a steak, which was awesome,” she said. Then, fork in her left hand, she speared a piece and lifted it to her mouth — one previously impossible movement at a time.
Read more →


