
GPs strike deal to help end ‘8am scramble’ for appointments

Patients will be able to book more appointments online and request to see their usual doctor under a new contract agreed with England’s GPs, the government has said.
Read more →
Patients will be able to book more appointments online and request to see their usual doctor under a new contract agreed with England’s GPs, the government has said.
Read more →
new video loaded:
Read more →
Amanda Pritchard, the first female chief executive of the NHS in England, is stepping down from the role.
Read more →
Baby milk formula should have plain packaging in hospitals, the regulator has said following a probe into the market.
Read more →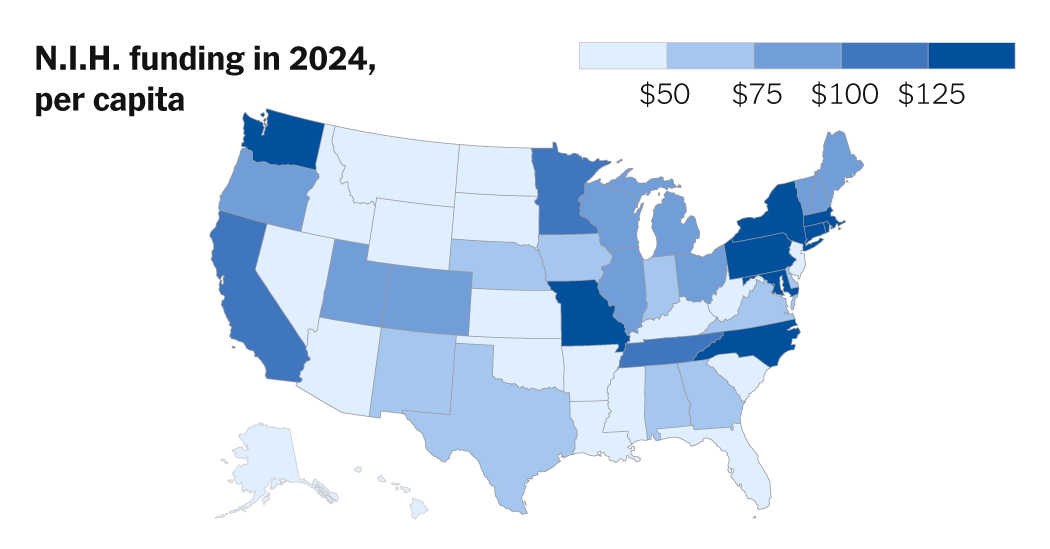
A proposal by the Trump administration to reduce the size of grants for institutions conducting medical research would have far-reaching […]
Read more →
45 minutes agoNick Triggle, Hugh Pym, Chloe Hayward, Vicki Loader & Jim ReedBBC News
Read more →
When Secretary of State Marco Rubio announced last month that lifesaving humanitarian work would be exempt from a freeze on foreign aid, global health workers breathed a collective sigh of relief.But a new directive has put such exemptions on hold.Several senior employees at the U.S.A.I.D. Bureau of Global Health received an email Tuesday telling them to “please hold off on any more approvals” pending further directions from the acting chief of staff, according to a copy reviewed by The New York Times.Senior officials at the Bureau of Humanitarian Assistance received similar instructions during a meeting this week, according to a person familiar with what transpired.For weeks, U.S.A.I.D. officials and the organizations, contractors and consultants who partner with them have struggled to continue the kind of work that Mr. Rubio promised to preserve — “core lifesaving medicine, medical services, food, shelter and substance assistance.”Some waivers have been issued to programs that fall under Mr. Rubio’s definition of “lifesaving” aid, but the payments system called Phoenix that U.S.A.I.D. relies on to disburse financial assistance has been inaccessible for weeks. That means even programs that received waivers have struggled to continue, according to multiple employees of U.S.A.I.D. and the partner organizations that rely on the funding they distributed.The State Department did not reply to a request for comment for this article.On Tuesday, Elon Musk, the billionaire tech entrepreneur empowered by President Trump to combat the agency, told reporters in the Oval Office that the administration had “turned on funding for Ebola prevention and for H.I.V. prevention.” But in reality, the Ebola funding and virtually all of the H.I.V. prevention funding remains frozen, according to two U.S.A.I.D. employees and several aid groups.We are having trouble retrieving the article content.Please enable JavaScript in your browser settings.Thank you for your patience while we verify access. If you are in Reader mode please exit and log into your Times account, or subscribe for all of The Times.Thank you for your patience while we verify access.Already a subscriber? Log in.Want all of The Times? Subscribe.
Read more →
22 hours agoAdam Eley and Alison Holt, social affairs editorBBC News
Read more →
22 minutes agoGetty ImagesHospitals in England have just had their busiest week of this winter so far.
Read more →