
Warning over the dangers of Botox parties
1 hour ago
Read more →
18 minutes ago
Read more →
13 minutes ago
Read more →
new video loaded:
Read more →
How Republicans could change the program. Republican leaders in Congress have directed the committee that oversees Medicaid to cut $880 billion from the next budget. They say these cuts aren’t necessarily aimed at Medicaid, the insurance program for 72 million poor and disabled Americans. The cuts could come from Medicare, for instance. But Trump has vowed not to touch that very popular program. And a sum this large can’t come from anywhere else.The Republican process is just getting started, and we don’t yet know how lawmakers will change the program. Most Medicaid money goes to states, so the best way to think about the proposal is as a cut to state budgets. State lawmakers could react by dropping coverage, raising taxes or slashing other parts of their budget. In today’s newsletter, I’ll explain a few possible scenarios.Spending overseen by the House Committee On Energy and Commerce
Read more →
31 minutes ago
Read more →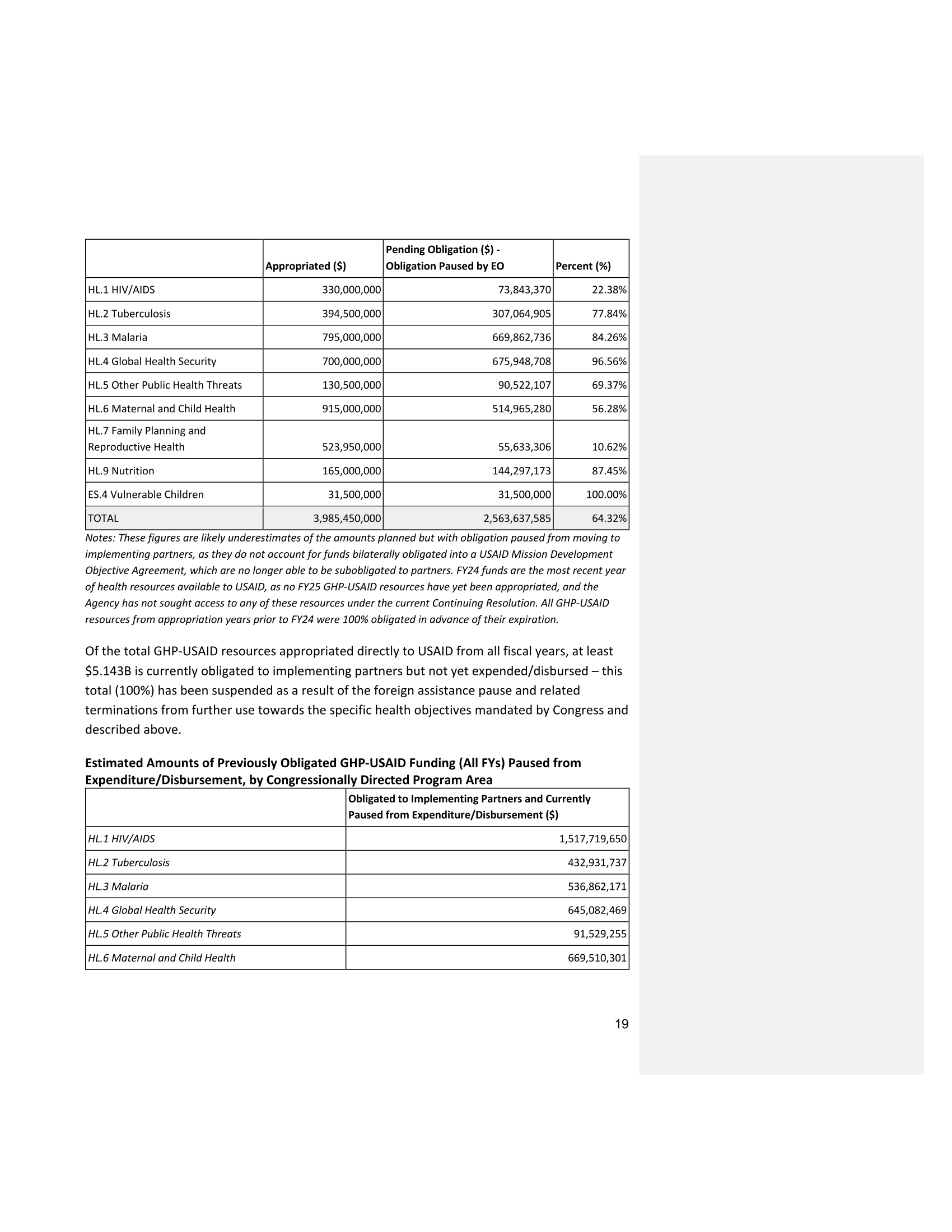
Pending Obligation ($) –
Appropriated ($)
Obligation Paused by EO
Percent (%)
HL.1 HIV/AIDS
HL.2 Tuberculosis
330,000,000
73,843,370
22.38%
394,500,000
307,064,905
77.84%
HL.3 Malaria
795,000,000
669,862,736
84.26%
HL.4 Global Health Security
700,000,000
675,948,708
96.56%
HL.5 Other Public Health Threats
130,500,000
90,522,107
69.37%
HL.6 Maternal and Child Health
915,000,000
514,965,280
56.28%
HL.7 Family Planning and
Reproductive Health
HL.9 Nutrition
ES.4 Vulnerable Children
523,950,000
55,633,306
10.62%
165,000,000
144,297,173
87.45%
31,500,000
31,500,000
100.00%
3,985,450,000
2,563,637,585
64.32%
TOTAL
Notes: These figures are likely underestimates of the amounts planned but with obligation paused from moving to
implementing partners, as they do not account for funds bilaterally obligated into a USAID Mission Development
Objective Agreement, which are no longer able to be subobligated to partners. FY24 funds are the most recent year
of health resources available to USAID, as no FY25 GHP-USAID resources have yet been appropriated, and the
Agency has not sought access to any of these resources under the current Continuing Resolution. All GHP-USAID
resources from appropriation years prior to FY24 were 100% obligated in advance of their expiration.
Of the total GHP-USAID resources appropriated directly to USAID from all fiscal years, at least
$5.143B is currently obligated to implementing partners but not yet expended/disbursed – this
total (100%) has been suspended as a result of the foreign assistance pause and related
terminations from further use towards the specific health objectives mandated by Congress and
described above.
Estimated Amounts of Previously Obligated GHP-USAID Funding (All FYs) Paused from
Expenditure/Disbursement, by Congressionally Directed Program Area
Obligated to Implementing Partners and Currently
Paused from Expenditure/Disbursement ($)
HL.1 HIV/AIDS
HL.2 Tuberculosis
HL.3 Malaria
HL.4 Global Health Security
HL.5 Other Public Health Threats
HL.6 Maternal and Child Health
1,517,719,650
432,931,737
536,862,171
645,082,469
91,529,255
669,510,301
19

Heat from the eruption in A.D. 79 was so intense that it vitrified the brain tissue of one unfortunate Herculaneum resident, a new study confirms.Five years ago Italian researchers published a study on the eruption of Mount Vesuvius in A.D. 79. that detailed how one victim of the blast, a male presumed to be in his mid 20s, had been found nearby in the seaside settlement of Herculaneum. He was lying facedown and buried by ash on a wooden bed in the College of the Augustales, a public building dedicated to the worship of Emperor Augustus. Some scholars believe that the man was the center’s caretaker and was asleep at the time of the disaster.In 2018, one researcher discovered black, glossy shards embedded inside the caretaker’s skull. The paper, published in 2020, speculated that the heat of the explosion was so immense that it had fused the victim’s brain tissue into glass.Forensic analysis of the obsidian-like chips revealed proteins common in brain tissue and fatty acids found in human hair, while a chunk of charred wood unearthed near the skeleton indicated a thermal reading as high as 968 degrees Fahrenheit, roughly the dome temperature of a wood-fired Neapolitan pizza oven. It was the only known instance of soft tissue — much less any organic material — being naturally preserved as glass.On Thursday, a paper published in Nature verified that the fragments are indeed glassified brain. Using techniques such as electron microscopy, energy dispersive X-ray spectroscopy and differential scanning calorimetry, scientists examined the physical properties of samples taken from the glassy fragments and demonstrated how they were formed and preserved. “The unique finding implies unique processes,” said Guido Giordano, a volcanologist at the Roma Tre University and lead author of the new study.The archaeological site of Herculaneum with Mount Vesuvius looming in the background.Pier Paolo PetroneForemost among those processes is vitrification, by which material is burned at a high heat until it liquefies. To harden into glass, the substance requires rapid cooling, solidifying at a temperature higher than its surroundings. This makes organic glass formation challenging, Dr. Giordano said, as vitrification entails very specific temperature conditions and the liquid form must cool fast enough to avoid being crystallized as it congeals.We are having trouble retrieving the article content.Please enable JavaScript in your browser settings.Thank you for your patience while we verify access. If you are in Reader mode please exit and log into your Times account, or subscribe for all of The Times.Thank you for your patience while we verify access.Already a subscriber? Log in.Want all of The Times? Subscribe.
Read more →