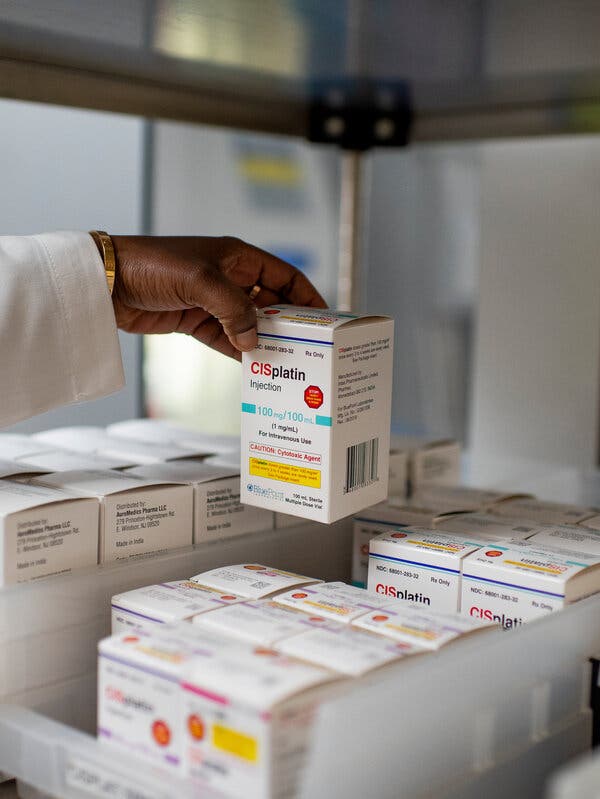
Aspartame is Possibly Linked to Cancer in Humans, the WHO Says

The F.D.A. and the powerful beverage industry protested the new findings, and a second W.H.O. group stood by its standard that the sweetener is generally safe.A World Health Organization agency declared on Thursday that aspartame, an artificial sweetener widely used in diet drinks and low-sugar foods, could possibly cause cancer.A second W.H.O. committee, though, held steady on its assessment of a safe level of aspartame consumption. By some calculations using the panel’s standard, a person weighing 150 pounds could avoid a risk of cancer but still drink about a dozen cans of diet soda a day.The declaration by a W.H.O. agency of a cancer risk associated with aspartame reflects the first time the prominent international body has weighed in publicly on the effects of the nearly ubiquitous artificial sweetener. Aspartame has been a contentious ingredient for decades.The International Agency for Research on Cancer, or I.A.R.C., said it based its conclusion that aspartame was a possible carcinogen on limited evidence from three observational studies of humans that the agency said linked consumption of artificially sweetened beverages to an increase in cases of liver cancer — at levels far below a dozen cans a day. It cautioned that the results could potentially be skewed toward the profile of people who drink higher amounts of diet drinks and called for further study.Still, people who consume high amounts of aspartame should consider switching to water or other unsweetened drinks, said Dr. Francesco Branca, director of the W.H.O. Department of Nutrition and Food Safety.But, he added: “Our results do not indicate that occasional consumption should pose a risk to most.”Concerns about rising global rates of obesity and diabetes as well as changing consumer preferences have resulted in an explosion of no- and low-sugar food and beverages. Aspartame, one of six sweeteners approved by U.S. regulators, is found in thousands of products, from packets of Equal to sugar-free gum, diet sodas, teas, energy drinks and even yogurts. It is also used to sweeten various pharmaceutical products.The U.S. Food and Drug Administration, which approved aspartame decades ago, on Thursday issued an unusual criticism of the global agency’s findings and reiterated its longstanding position that the sweetener is safe. In a statement, the F.D.A. said it “disagrees with I.A.R.C.’s conclusion that these studies support classifying aspartame as a possible carcinogen to humans.”The F.D.A. also said that “aspartame being labeled by the W.H.O. as ‘possibly carcinogenic to humans’ does not mean that aspartame is actually linked to cancer.” The F.D.A. declined to make any of its experts available for interviews to discuss the agency’s specific concerns.But its salvo against the international organization was sure to ignite further debate in Europe — where the sweetener is still deemed safe — and renew review in the United States. And the dueling global agencies’ pronouncements are likely to fuel confusion among consumers.The W.HO. has occasionally been out of step with other authorities on potential cancer risks, like glyphosate, and later led the way toward establishing that it was dangerous to human health. The international body’s designation of a cancer link to that ingredient in Roundup, a weed killer, became the stepping stone for lawsuits against the makers of the herbicide.Around the world, the powerful beverage industry has fought long and hard against any regulatory or scientific finding that tied artificial sweetener use to risks of cancer or other health problems. Aspartame is only the latest battleground for multinational companies to push back against new studies or potential links to health risks.Researchers in the Cesare Maltoni Cancer Research Center in Bologna, Italy, in 2006. Italian researchers conducting rodent studies from 2005 to 2010 rekindled the debate over aspartame.Pigi Cipelli for The New York Times“Aspartame is safe,” Kevin Keane, interim president of the American Beverage Association, said in a statement. He cited the dueling W.H.O. announcements, singling out the second panel, the Joint Expert Committee on Food Additives, that performed a concurrent review and left its recommended daily intake amount unchanged. It also deemed the evidence for cancer in humans “not convincing,” a W.H.O. summary shows.“After a rigorous review, the World Health Organization finds aspartame is safe and ‘no sufficient reason to change the previously established acceptable daily intake,’” Mr. Keane said. “This strong conclusion reinforces the position of the F.D.A. and food safety agencies from more than 90 countries.”Coca-Cola referred questions to the American Beverage Association and PepsiCo did not respond to requests for comment.The safety of sugar replacements, including the decades-old science dispute over the use of saccharin in the diet drink Tab, has been heavily scrutinized. Once linked to bladder cancer in rats, Congress mandated further study of saccharin. Since then, according to the F.D.A., 30 studies showed the rodent results did not apply to humans; U.S. officials removed saccharin from a list of potential carcinogens. More recently, other sweeteners have come under scrutiny for their ties to possible health risks.At the center of the dispute over aspartame are rodent studies from 2005-2010 by Italy-based researchers that showed a link to cancer. The F.D.A. has dismissed the long-debated studies as “compromised.”Dr. William Dahut, chief scientific officer of the American Cancer Society, which led one of the key studies the W.H.O. relied on, said the findings should be considered alongside the W.H.O.’s report earlier this year that indicated artificial sweeteners offered no help in achieving weight loss or protection from other chronic conditions.He said there was little evidence now to suggest a daily Diet Coke would elevate the risk of cancer, adding that “more research is needed.” Overall, he said, the science was more definitive on reducing cancer risk by avoiding tobacco, alcohol, processed meat and excess body weight.The I.A.R.C. said it could not rule out the possibility that the studies linking aspartame to liver cancer were a result of chance or other factors associated with drinking diet soda.The W.H.O.’s cancer agency has four categories: carcinogenic, probably carcinogenic, possibly carcinogenic and no classification. Those levels reflect the strength of the science rather than how likely the substance is to cause cancer.The other W.H.O. group on food additives recommended that daily consumption should be below 40 milligrams of aspartame per kilogram of a person’s weight — slightly lower than the suggested U.S. level of 50 milligrams.The F.D.A. said it estimated that a person weighing 132 pounds would need to consume 75 packets of aspartame sweetener to reach the threshold of exposure to a potential risk.For its review of aspartame, the I.A.R.C. convened 25 cancer experts from 12 nations in Lyon, France, to conduct the review of existing studies. It concluded that there was limited evidence for cancer in humans based on three studies linking artificially sweetened drinks to increases in hepatocellular carcinoma, the most common type of liver cancer.One study in 2016 was led by W.H.O. officials, who looked at nearly 500,000 people in Europe who were followed for about 11 years. The study tracked participants’ juice and soft drink intake and the relationship to liver and bile duct cancers. It examined those who drank artificially sweetened soft drinks and found that each additional serving of diet soft drink a week was associated with a 6 percent increased risk of liver cancer.A U.S. study published last year by researchers from Harvard, Boston University and the National Cancer Institute examined sweetened beverage consumption reported by people on questionnaires and cancer case registries. Researchers found an elevated risk of liver cancer in people with diabetes who said they consumed two or more artificially sweetened sodas a day. That study found no increase in liver cancer among diet soda drinkers who did not have diabetes.The F.D.A., which approved aspartame decades ago, responded strongly to the I.A.R.C.’s conclusions.Andrew Harnik/Associated PressA third study, led by the American Cancer Society, examined the use of beverages sweetened by sugar and artificial sweeteners and cancer death data. It found a 44 percent increase in liver cancer among men who never smoked and drank two or more artificially sweetened drinks a day. Even adjusting for high body mass — in itself a cancer risk factor — the men had a 22 percent increase in risk, data in a supplement to the study shows.The American Beverage Association, which represents Coca-Cola and PepsiCo, has been vocal in saying that the W.H.O.’s food additive panel — not the cancer experts — should be the lead authority evaluating aspartame.In recent weeks, the beverage industry trade group has financed a new coalition led by Alex Azar, an appointee of former President Donald J. Trump, and Donna Shalala, an appointee of former President Bill Clinton. Both Mr. Azar and Ms. Shalala were former secretaries of the Department of Health and Human Services. In an opinion article in Newsweek earlier this month, the two embraced the F.D.A.’s position on the safety of aspartame, and called the agency “the world’s gold standard for independent regulatory bodies.”The trade group had previously contested another review of aspartame’s potential links to cancer in California. In 2016, a state committee discussed reviewing aspartame, but it went no further.California officials said this week that the state could review the latest W.H.O. decision.Besides aspartame, the W.H.O.’s cancer agency has deemed other possible carcinogens to range from the seemingly benign, like Ginkgo biloba extract and aloe vera leaf extract, to the more concerning, like gasoline exhaust and perfluorooctanoic acid, the most common of the industrial chemicals known as per- and polyfluoroalkyl substances, or PFAS, that has recently been subject to billion-dollar settlements over drinking water contamination.In deeming aspartame a possible carcinogen, the I.A.R.C. also dipped into one of the central controversies of aspartame research. It concluded that there was some evidence for cancer in lab animals based on studies performed by the Ramazzini Institute in Italy, citing the group’s finding of increased tumors in aspartame studies from the mid-2000s. Based on concerns over the group’s methods and interpretations, though, the findings were deemed limited.For its part, the Ramazzini Institute said in 2021 that its work on aspartame was validated and that its earlier findings were “savagely attacked by the chemical manufacturing and processed food industries and by their allies in regulatory agencies.”Dr. Branca of the W.H.O. responded to questions about the need for an I.A.R.C. review during a news conference on Wednesday, saying that 10 million people die of cancer each year. “So there’s a societal concern that our organization needed to respond to,” he said.He said the results demonstrated a clear need for further high-quality research.“We’ve in a sense raised a flag here, indicating that we need to clarify much more in the situation,” Dr. Branca said. “It is not something which we can dismiss at this moment.”Julie Creswell contributed reporting to this article.
Read more →