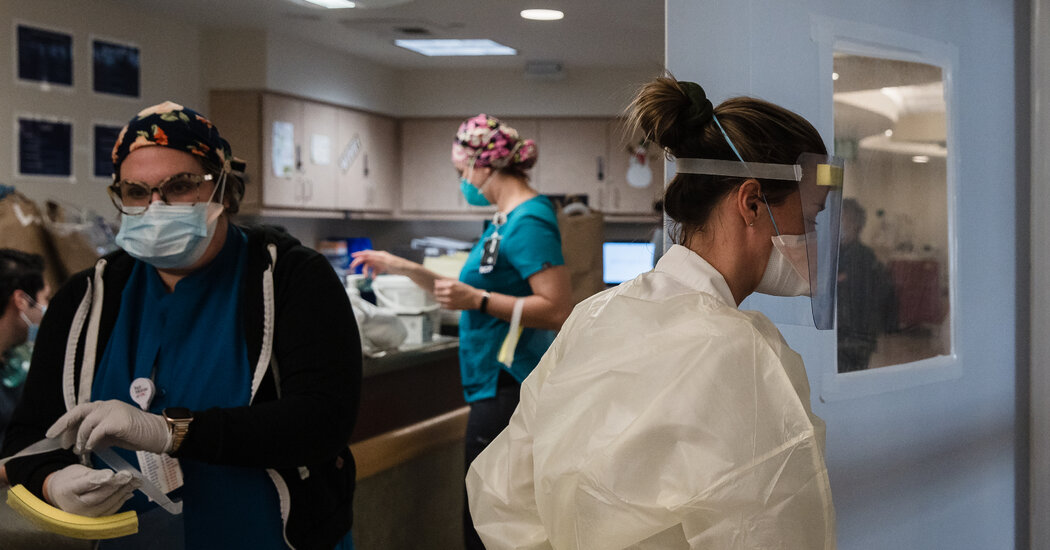
Even with vaccines, many older people and their relatives are weighing how to manage at-home care for those who can no longer live independently.At 86, Diane Nixon, living in an apartment at the back of a daughter’s house, no longer drives and has trouble getting around.When her health worsened last year before the coronavirus pandemic, she and all four of her daughters talked about whether a nursing home would be the next step. She worried that she had become a burden to her children.“She was very adamant about not wanting her daughters to be caregivers,” said Jill Cooper, one of her daughters, who lives nearby in the Pittsburgh area.But as infections began to tear through nursing homes across the country, killing tens of thousands of residents last year, Ms. Nixon and her family realized a group home was no longer a viable choice. Especially after most of them barred visitors to help contain outbreaks.“Not to be able to see her was not an option for us,” Ms. Cooper said, so the family contacted a local home health agency to hire someone to help her during the day.“It made us look at an alternative that we might not have looked at as hard,” she said.The pandemic’s toll on nursing homes drove occupancy down significantly — not just from the 132,000 deaths but also because of a decline in admissions. The 14,000 skilled nursing facilities in the United States now have on average a vacancy rate of slightly more than 25 percent, according to figures from the National Investment Center for Seniors Housing & Care.But as immunization campaigns inside them began taking priority in the winter this year, with nearly three million residents and staff members fully vaccinated, the outlook improved somewhat. Nursing homes point to the steep decrease in Covid-related deaths, saying they have dropped by 91 percent since December.While the industry has received $21 billion in federal funding under the CARES Act as part of congressional efforts to help health care facilities during the pandemic, nursing homes are lobbying for more federal aid to cover the higher cost of personal protective equipment, testing and staffing at their facilities. They say that they are losing tens of billions of dollars in revenue because of the pandemic and that many homes are at risk of closing.But the deaths of so many elderly residents, captive in those homes, has deepened levels of anxiety and guilt among many families planning the next phase of care for an aging relative. Experts say rethinking the purpose of nursing homes is long overdue.Even before the pandemic began 14 months ago, nursing homes had become the source for rampant, antibiotic-resistant infections. The facilities also faced systemic problems like high turnover among nursing home staff and the gaming of the federal government’s rating system, which made it hard for families to judge the quality of homes.For years, federal health officials and some insurers have tried to encourage more stay-at-home care, and the pandemic has created a sense of urgency.“It’s really changed the paradigm on how older adults want to live,” said Dr. Sarita Mohanty, the chief executive of the SCAN Foundation, a nonprofit group focused on issues facing older adults. The vast majority of those adults would prefer to stay at home as they age, she said.“What’s happened is a welcome sort of market correction for nursing homes,” said Tony Chicotel, a staff attorney for California Advocates for Nursing Home Reform in San Francisco. Some families, he said, “ended up agreeing to a nursing home without giving it a lot of deliberation.” But after trying home care during the pandemic, many families found keeping an older relative at home was a viable alternative, he said.Nursing homes rose from the almshouses in England and America that cared for the poor. In the United States, passage of the Social Security Act in 1935 provided money for states to care for the elderly. Thirty years later, the Medicaid program expanded funding, making long-term care homes central to elder care, said Terry Fulmer, the president of the John A. Hartford Foundation, an advocacy group for older adults. “If you pay the nursing homes, that’s where you go,” Dr. Fulmer said.It wasn’t until the 1970s that some programs began to pay for home care, and the number of nursing home residents nationwide started to slowly decline, with occupancy levels in recent years flattened to about 80 percent, according to data from the Kaiser Family Foundation.New technology makes it easier to monitor someone at home, said Dr. Fulmer, who thinks the pandemic might be a “tipping point.”Heidi Dolan, left, and Jill Cooper, Ms. Nixon’s daughters. They have not ruled out eventually placing Ms. Nixon in a nursing home. “We’re continuing the journey,” Ms. Cooper said.Kristian Thacker for The New York TimesBeth Kreisman, a nurse who works at Debra D. Feldman & Associates in Buffalo Grove, Ill., helping families navigate these issues, faced the same dilemma with her stepmother, now 89. Her stepmother had been showing signs of dementia, and a hospital stay last spring “took a lot out of her,” Ms. Kreisman said.“She couldn’t go home by herself,” she said. “We were really in a quandary if she should go to skilled nursing or go home with a caregiver.”But concern about her contracting the virus at a facility persuaded the family to opt for home care. “We were absolutely convinced that if she got Covid, she would die,” Ms. Kreisman said.Now that her stepmother is vaccinated, the family has renewed discussions about whether she would be best served in a nursing home. Her stepmother doesn’t want to leave the home where she spent decades with Ms. Kreisman’s late father. “In her mind, if she moves out of her place, then she is leaving my dad,” she said.“We’ve decided for the time being to keep her home,” she said. Many of her clients are also choosing home care in lieu of a nursing home.“I think people are going to be more cautious and ask more questions before they place a loved one in a nursing home or choose one to go to themselves,” said Lori O. Smetanka, the executive director for the National Consumer Voice for Quality Long-Term Care, a nonprofit group. “People are still worried, to some extent, about their safety.”While the availability of a Covid vaccine has lessened the risk of a resident becoming ill, some residents and staff members are refusing to be vaccinated, making the environment still potentially dangerous. In Kentucky, an unvaccinated worker recently set off an outbreak, according to a study released last month by the Centers for Disease Control and Prevention.And some individuals may not need nursing home care. Debra Feldman, the founder of the Chicago agency, said she made the decision to have one client with dementia leave the facility where she was recovering from surgery for a broken hip because of the coronavirus restrictions imposed last spring.“It was really nice outside. She was being shut in her room, and she couldn’t understand what was going on,” said Ms. Feldman, who said her client was becoming increasingly agitated. The nursing home would not allow her to go outside on the patio.The woman, in her mid-80s, recovered well at home. “Now she’s walking without a walker,” Ms. Feldman said. “She is pretty solid on her feet.”The backyard of Ms. Dolan’s home, where Ms. Nixon has an apartment adjoining an outdoor sitting area.Kristian Thacker for The New York TimesBut many people don’t have a choice because of their financial situation or physical needs. “There’s limited wiggle room in avoiding nursing home care,” said Richard Mollot, the executive director of the Long Term Care Community Coalition, a nonprofit group in New York. “You’re not given a lot of time and choices when you leave the hospital,” he said.And many families know circumstances can change. Ms. Nixon’s family has not ruled out some day having her move into a nursing home. “We’re continuing the journey,” Ms. Cooper said, emphasizing that they still viewed long-term nursing homes positively.Home care costs can be prohibitive. If a person is reliant on Medicaid, the federal-state program, what services are available within the community or at home vary widely, depending on the individual state. In some places, paid home care is capped. “We are already seeing that people with low incomes have fewer choices because of the way the system is structured,” Ms. Smetanka said.The Biden administration has proposed spending $400 billion to address some of the gaps in long-term care by providing more funding under Medicaid for these alternatives, but prospects for President Biden’s $2 trillion package are unclear.In some areas of the country, staff shortages may also limit the available options, said Liz Barlowe, the former president of the Aging Life Care Association, a nonprofit representing senior care professionals. Even with seemingly low occupancy rates, nursing homes may be slow to accept new long-term residents because they do not have enough staffing, and home health agencies have difficulty finding enough aides if people need round-the-clock care. “That is a huge challenge, not only for facilities but also home care,” said Ms. Barlowe, who advises families in Seminole, Fla.Still, she says she has sensed a shift in views on long-term care among families, even as some of the worst of the experiences in nursing homes fade.The crisis laid bare how poorly equipped many facilities were to handle a pandemic, she said. It also underscored that the industry needs to make fundamental changes to restore the confidence of the country.“The damage is done,” Ms. Barlowe said. “Now we all know it can happen. We need to be looking at system change.”
Read more →